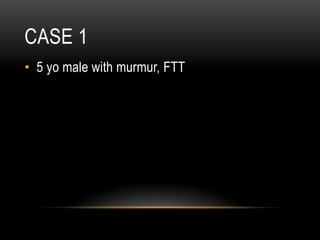
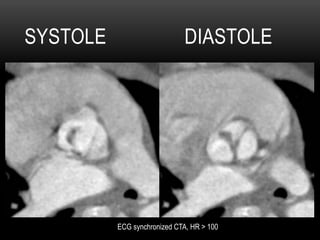
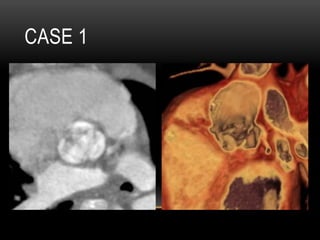
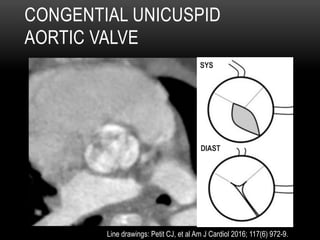
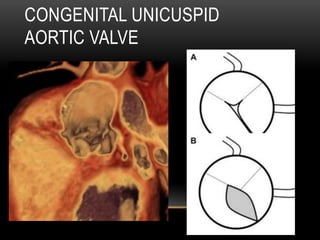
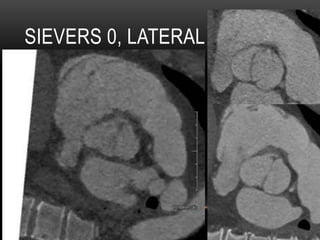
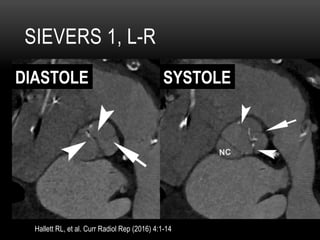
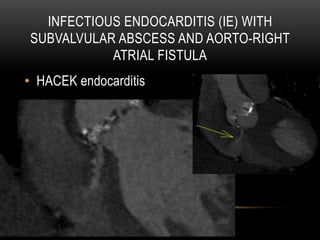
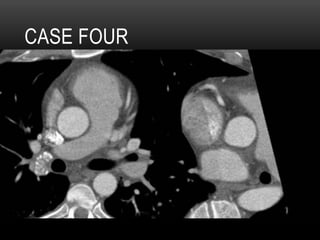
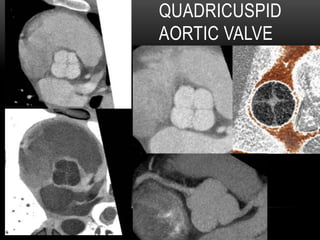
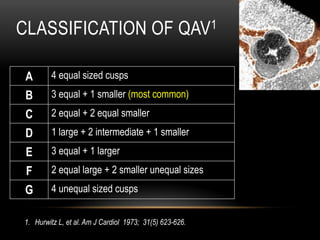
This document summarizes key points from a presentation on various congenital heart defects assessed by ECG-synchronized cardiac CT angiography. It discusses cases of unicuspid aortic valve, bicuspid aortic valve, infectious endocarditis with a subvalvular abscess and fistula, and quadricuspid aortic valve. For each case, it provides imaging findings and highlights important associated clinical features, complications, classifications where relevant, and management considerations for these congenital valve abnormalities.