Download to read offline








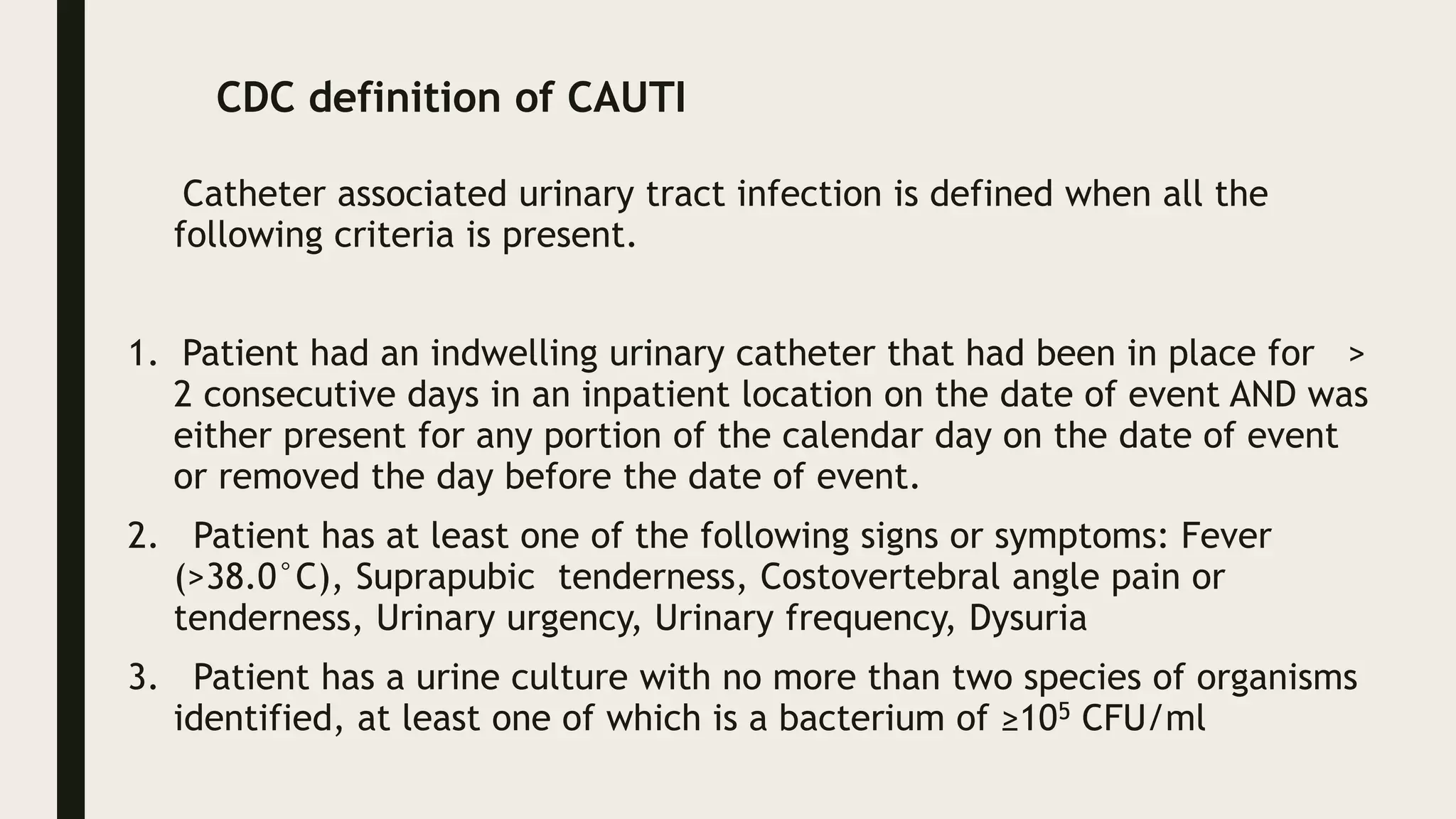















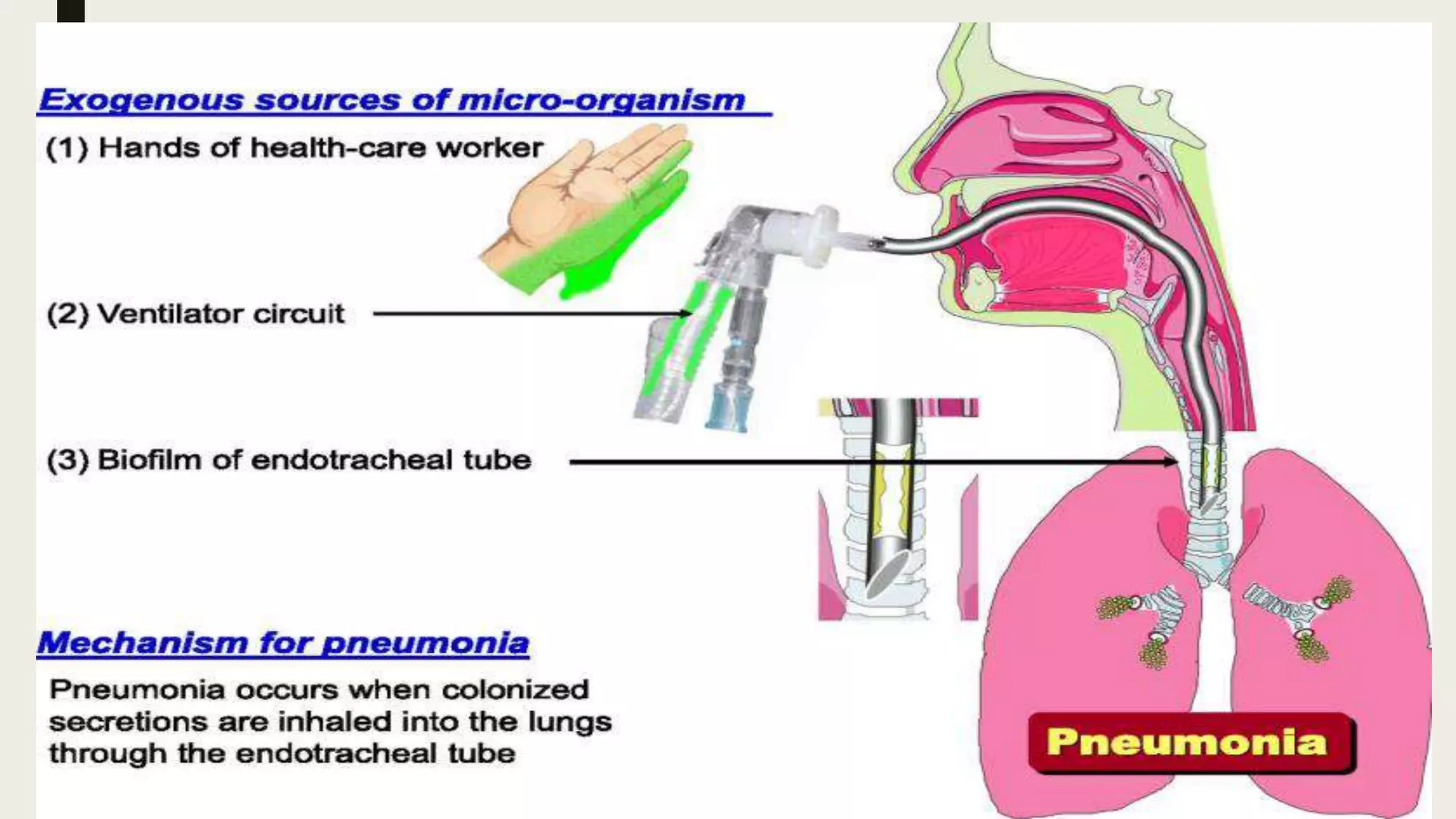
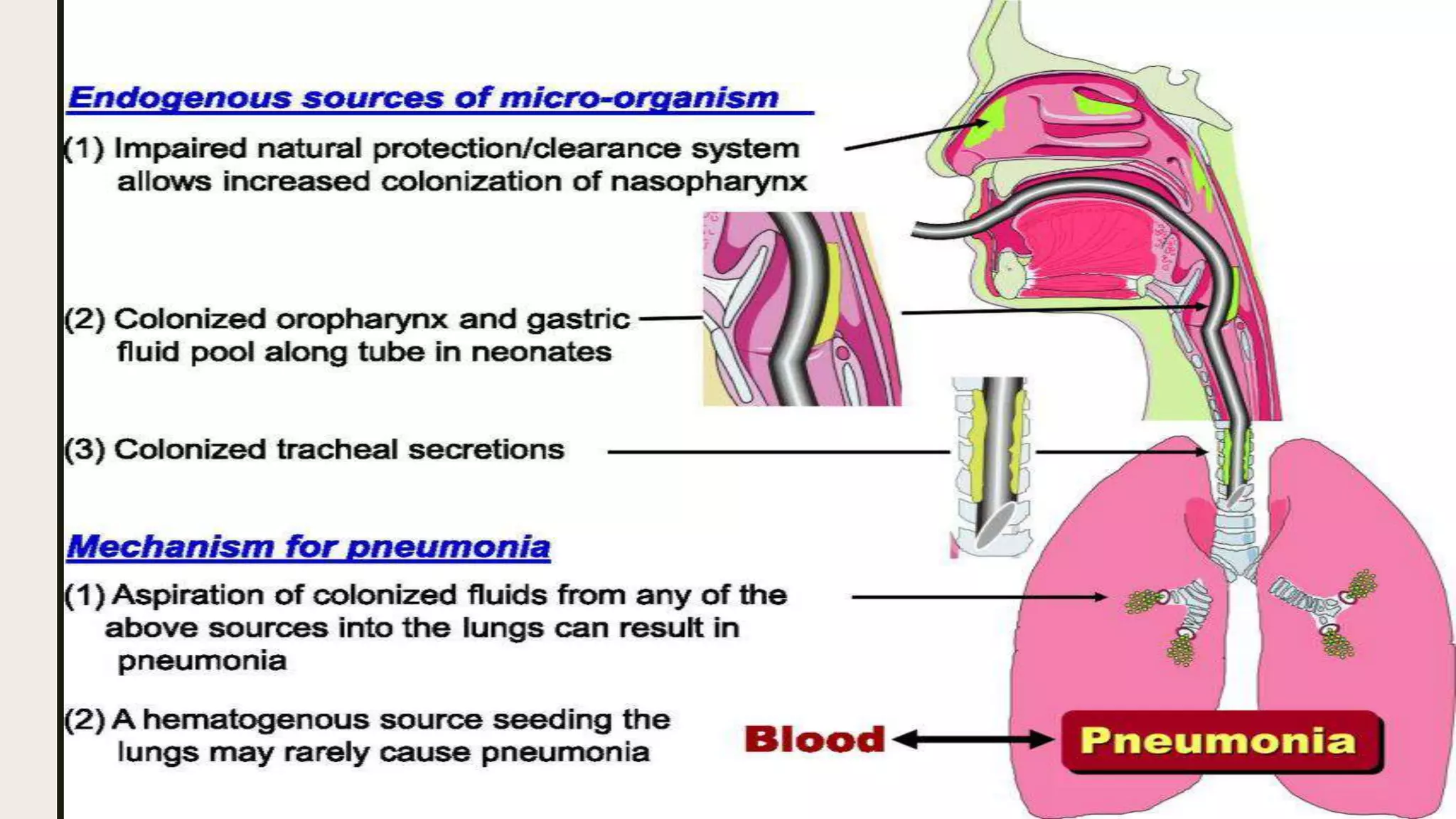
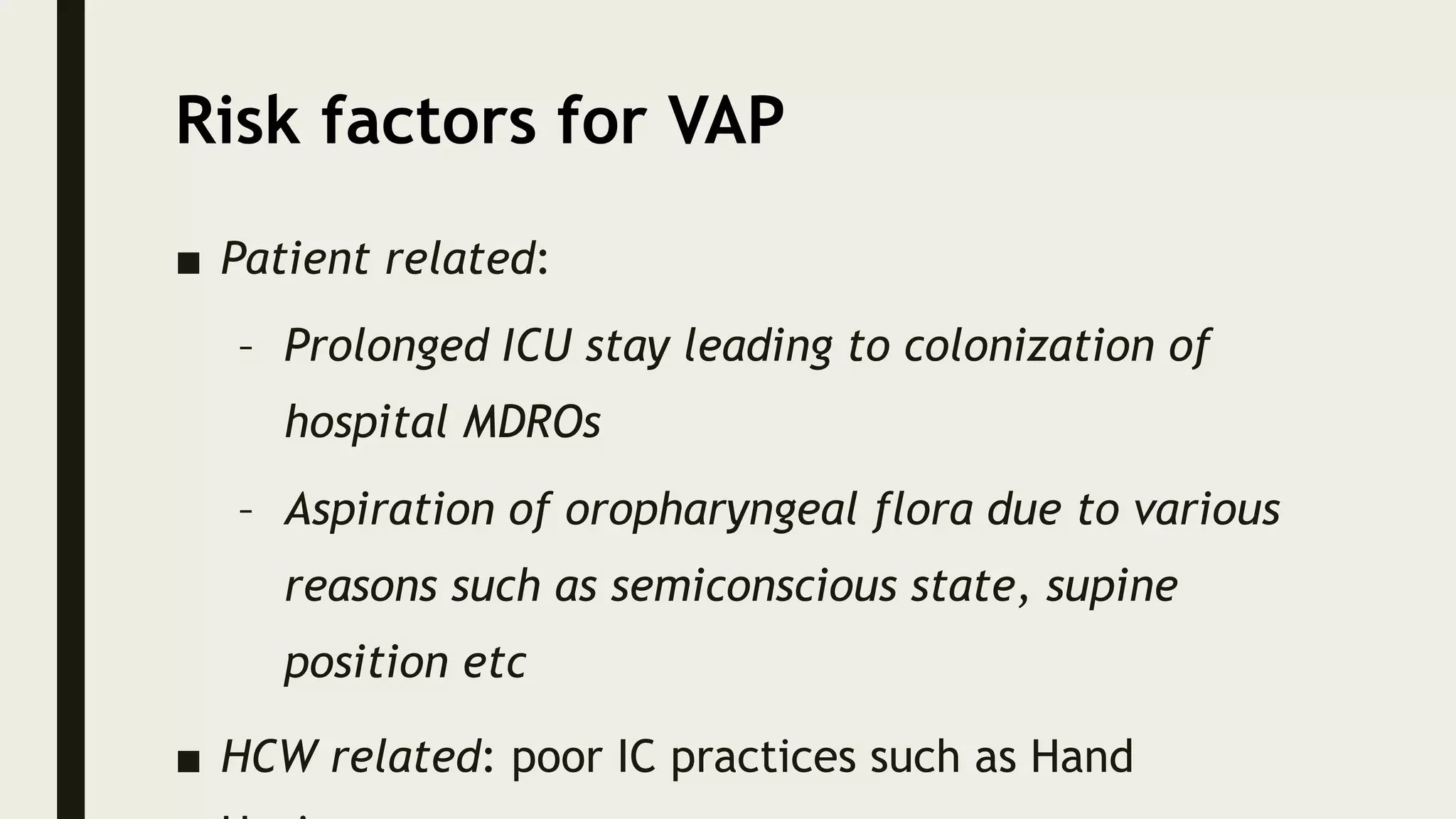














Health care-associated infections (HAIs), also called nosocomial infections, are infections patients acquire during the course of receiving treatment for other conditions within a healthcare setting. The most common types of HAIs are catheter-associated urinary tract infections, central line-associated bloodstream infections, ventilator-associated pneumonia, and surgical site infections. HAIs can increase patient suffering and mortality, prolong hospital stays, and increase healthcare costs. Proper hand hygiene, use of personal protective equipment, sterilization of equipment, judicious antibiotic use, and multimodal strategies are important for preventing the spread of HAIs within healthcare facilities.