Downloaded 679 times

















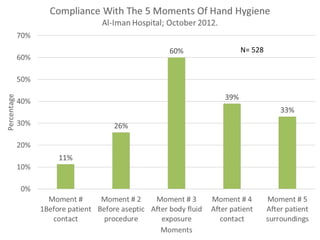








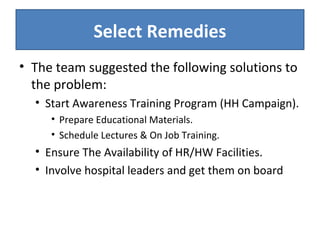


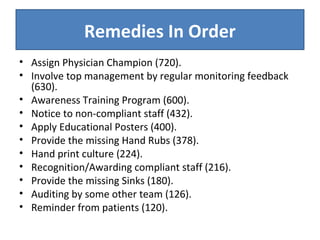
























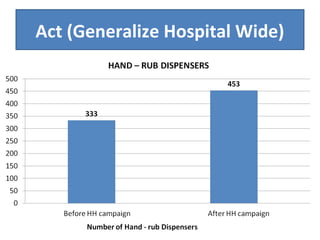




The document describes a quality improvement project to increase hand hygiene compliance at a hospital. Baseline data showed compliance was only 26%. A team analyzed the problem and identified solutions. These included an awareness training program, educational materials, ensuring hand hygiene supplies, and involving leaders. Regular audits and feedback to staff on compliance will also be implemented. The plan is to improve compliance to 90% by March 2014 through these multi-pronged interventions.



































































