This document provides an overview of treating sepsis in 8 steps:
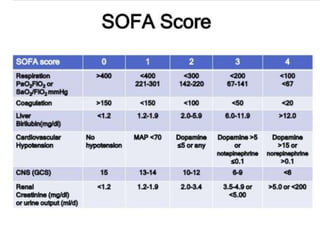
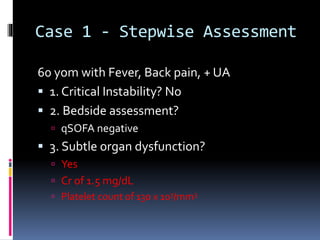
1) Rapidly assess for critical instability and signs of organ dysfunction
2) Administer empiric fluids and perform ultrasound exams to identify potential infection sources
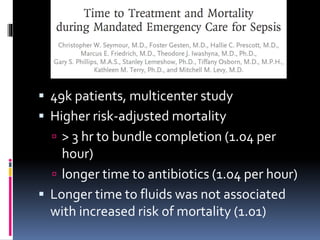
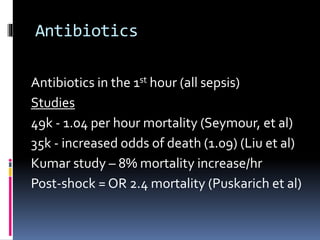
3) Administer early, broad-spectrum antibiotics within 1 hour
4) Identify and control infection sources
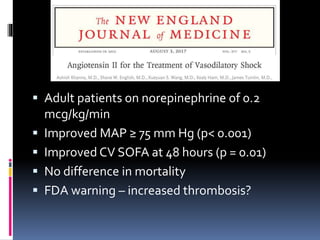
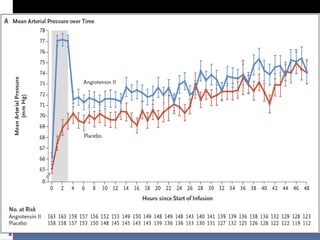
5) Understand appropriate vasoactive medications
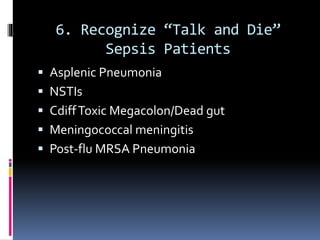
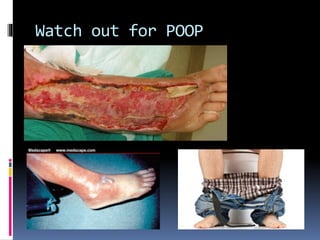
6) Recognize patients that deteriorate rapidly
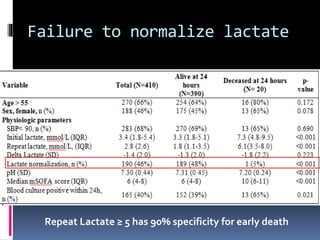
7) Use lactate levels to guide resuscitation but recognize limitations
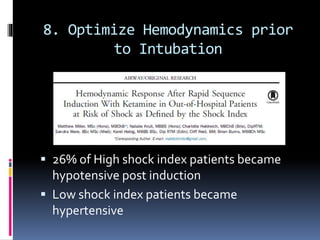
8) Optimize hemodynamics prior to intubation for shock patients
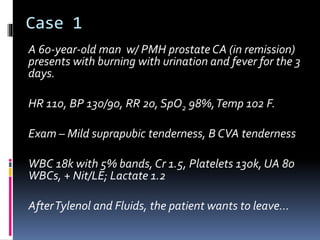
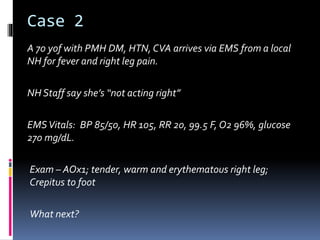
Two case studies are then presented and managed using the stepwise approach.