






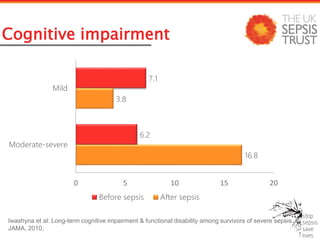

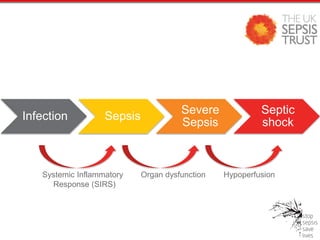
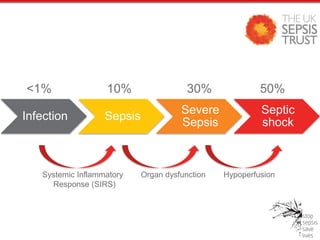
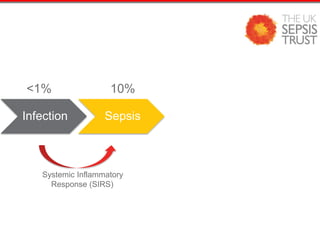





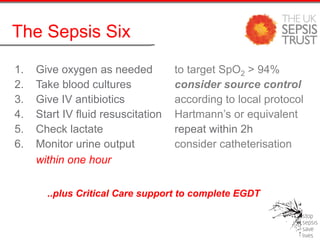

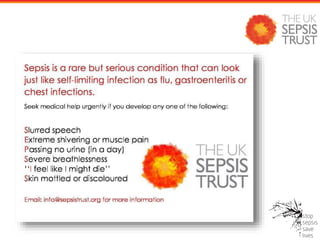


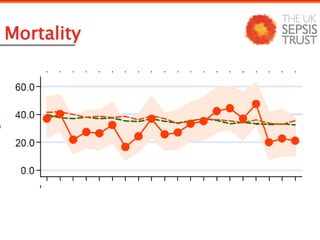



1) Sepsis is a life-threatening condition that arises when the body's response to infection causes injury to its own tissues and organs. Left untreated, sepsis can lead to septic shock, multiple organ failure, and death. 2) Early recognition and treatment of sepsis is key to reducing mortality. The "Sepsis Six" bundle of interventions should be completed within one hour for patients with sepsis, including administering oxygen, antibiotics, fluids, and monitoring lactate levels and urine output. 3) Sepsis can cause long-term cognitive and physical impairment in survivors. A study found that 16.8% of severe sepsis survivors had moderate to severe cognitive impairment after recovering.













































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















