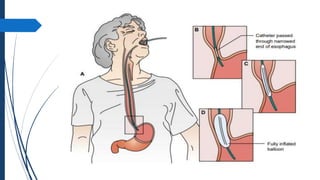
The document discusses disorders of the gastrointestinal system, beginning with a review of the anatomy and physiology of the GI tract. It describes the components and functions of the upper and lower GI tract. Key diagnostic tests are outlined including barium swallow, upper endoscopy, and colonoscopy. The disorder Achalasia is summarized, noting its causes, symptoms of dysphagia and chest pain, and treatments including medications to decrease LES pressure and forceful dilation.


















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















