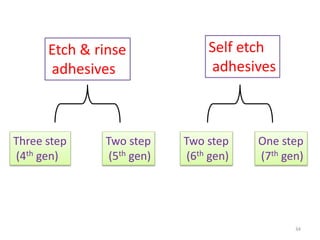
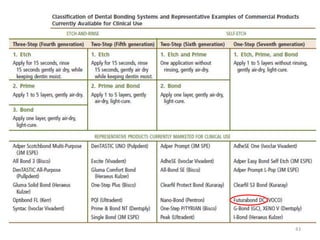
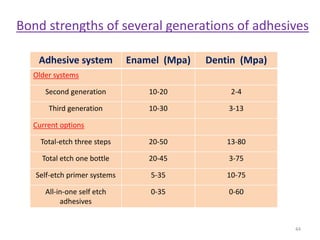
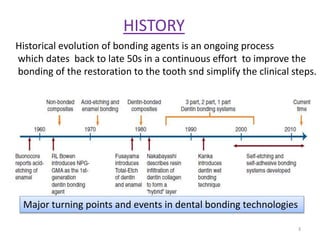
The document provides a historical perspective and current status of dental bonding agents. It discusses how bonding agents have evolved over generations from early calcium ion-based first generation agents with low bond strengths to today's multi-step etch-and-rinse and single-step self-etch adhesives. Current adhesives can achieve bond strengths of 20-50 MPa to enamel and 13-80 MPa to dentin. While newer single-step adhesives offer simplicity, their long-term performance is still being evaluated compared to multi-step systems. Proper technique remains important for clinical success with any bonding agent.
![COMPONENTS
Irrespective of the number of bottles or components, a typical
dentin bonding system includes :
- etchant - relatively strong acids (pH:1-2)
-removes smear layer
- gel (colloidal silica) – precise placement
-adhesive bisGMA, UDMA
- primer - maintains expanded collagen network
-hydrophillic monomers (phosphate, carboxylic
acid, esters) in solvents. [HEMA , 4-META]
- solvents used for primers (water, ethanol & acetone)
- initiators (photo ,chemical or dual cure)
- fillers silica(40nm)- reinforce
- other ingredients - glutaraldehyde - desensitizer
- MDPB & parabene – AMA
- F and CHX (prevents collagen degradation)
7](https://image.slidesharecdn.com/bondingagents-niraj-170226060142/85/Bonding-agents-IN-DENTISTRY-7-320.jpg)