Downloaded 307 times
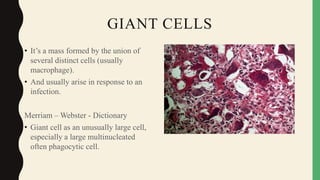
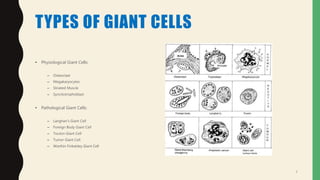
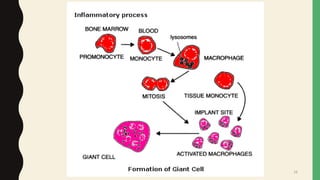
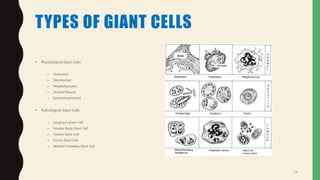
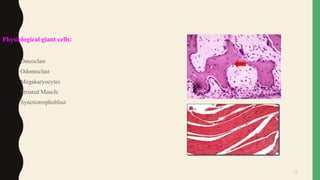
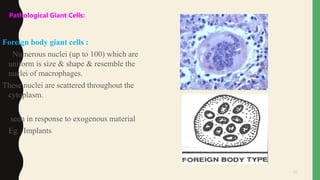


- Giant cells are large multinucleated cells formed by the fusion of macrophages in response to infection or foreign material. - There are physiological giant cells like osteoclasts and pathological giant cells seen in conditions like tuberculosis. - Pathological giant cells include foreign body giant cells, Langhans giant cells, and tumor giant cells. - Giant cells form through the fusion of macrophages mediated by cytokines, adhesion molecules, and oxidative stress. Nuclei and inclusion bodies can provide clues to the etiology of giant cell formation.























































































