Download as PDF, PPTX
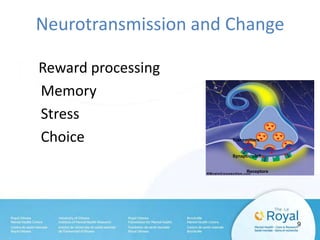
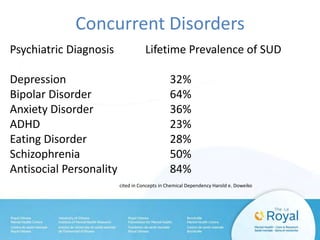
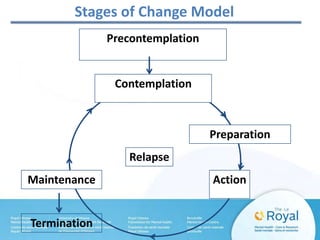

The document discusses addiction from multiple perspectives: - Addiction involves biological, psychological, and social factors that result in long-term brain changes and compulsion to use substances despite harm. It is considered a chronic disease by medical organizations. - Most people seeking treatment for substance use disorders or mental illness also have a concurrent or co-occurring disorder. Treatment aims to stabilize the individual, help them understand their disease and develop relapse prevention skills. - Recovery is a lifelong process of maintaining abstinence through structure, managing co-occurring issues, and reintegrating into family and community life with support. Understanding addiction helps individuals and families.























































































