Download to read offline


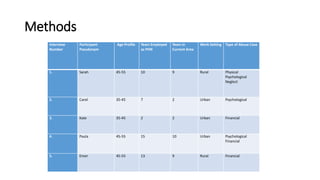
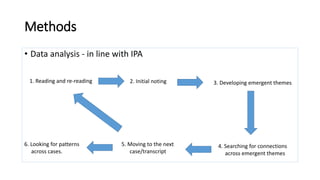
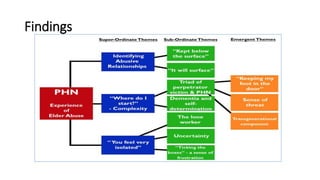

This study explored public health nurses' experiences with identifying and managing cases of elder abuse perpetrated against community-dwelling older adults with dementia. Through interviews with 5 public health nurses, the study found identifying hidden abusive relationships was complex, due to issues like capacity assessments and lack of support. The nurses experienced ethical challenges in balancing the needs of clients and families. They felt isolated in their role and uncertain without supervision or multidisciplinary collaboration. The study concludes public health nurses need more education, clinical supervision, and strengthened legislative frameworks to safely support vulnerable elders experiencing abuse.











































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





