




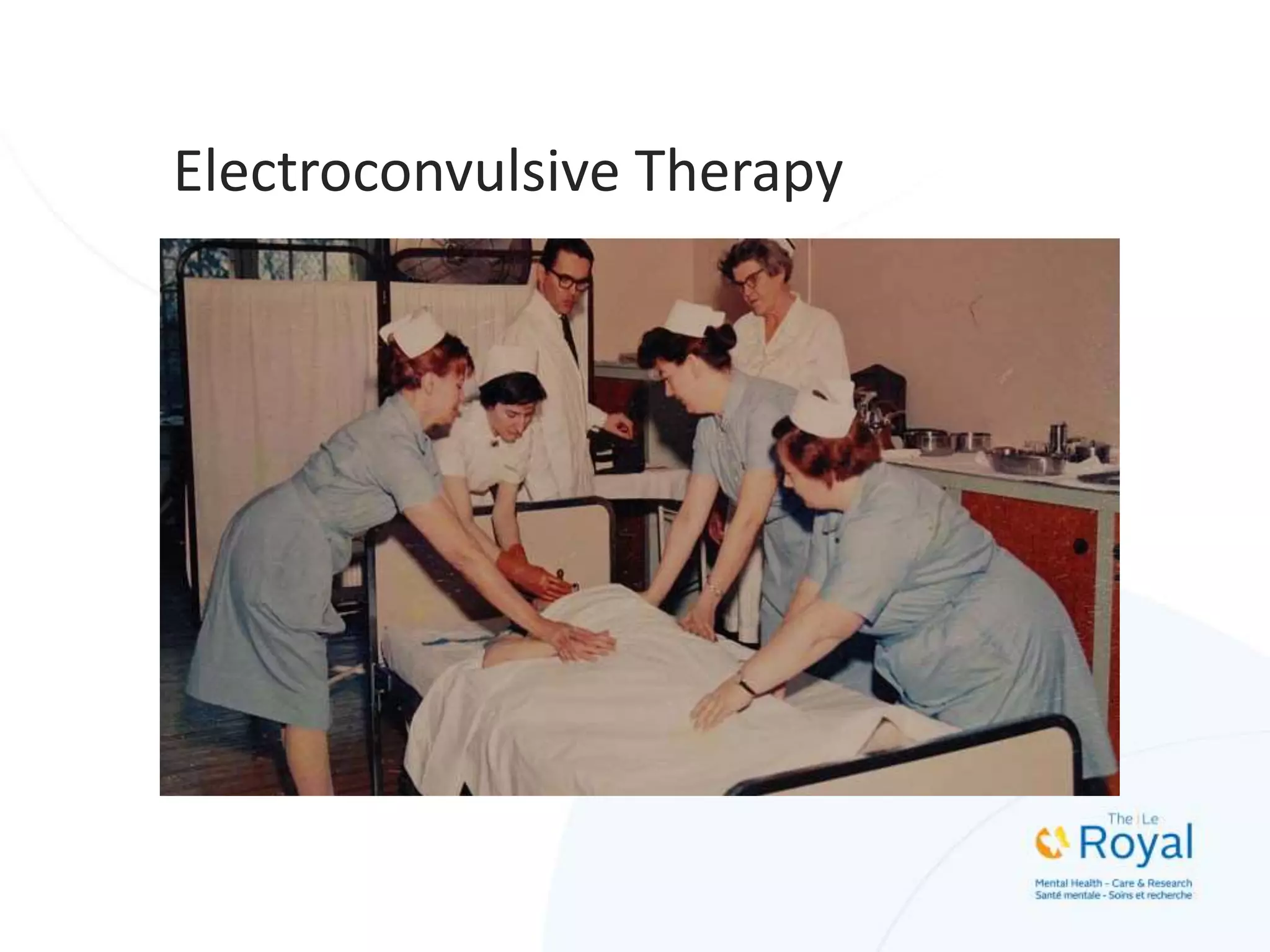
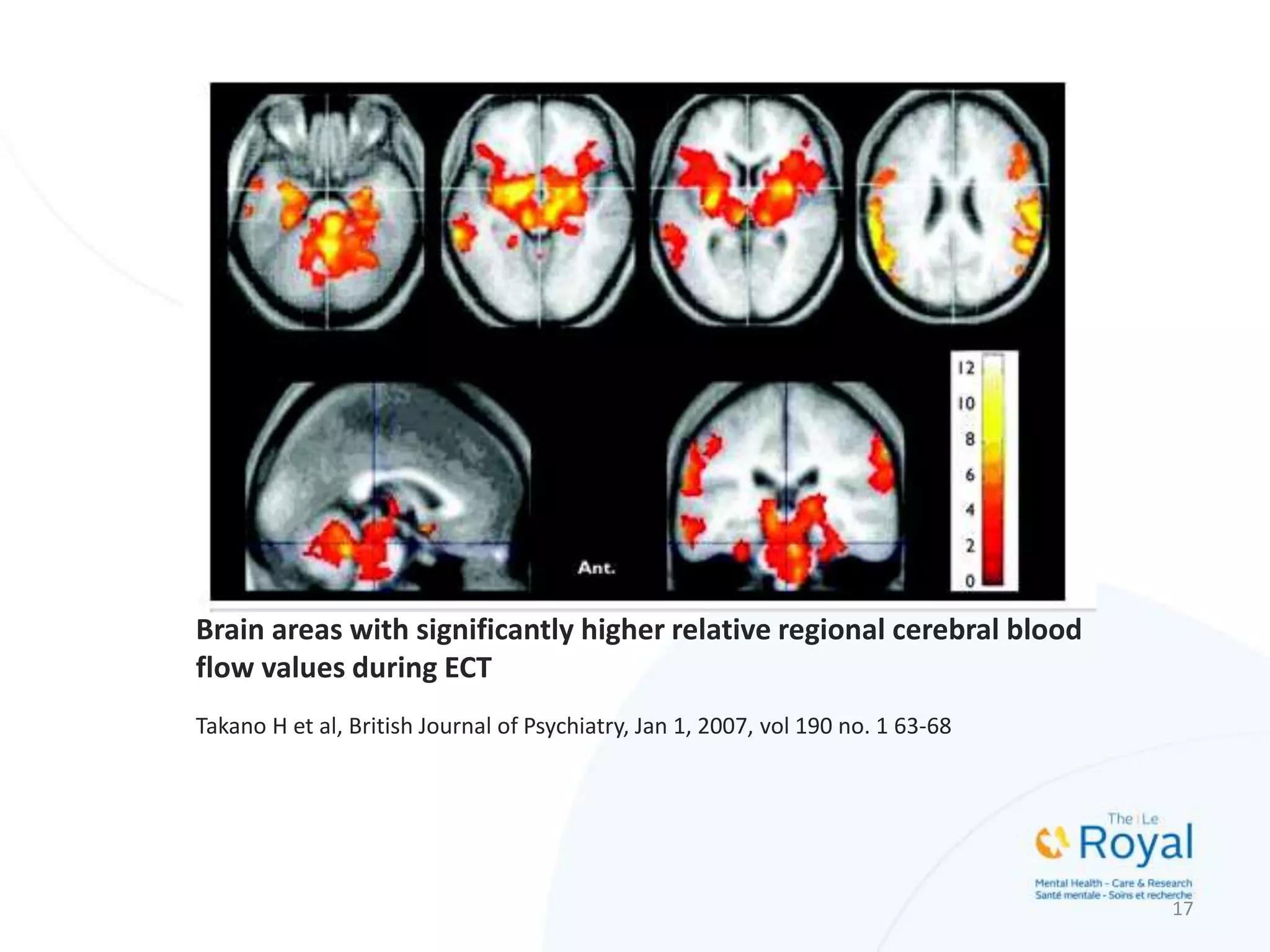
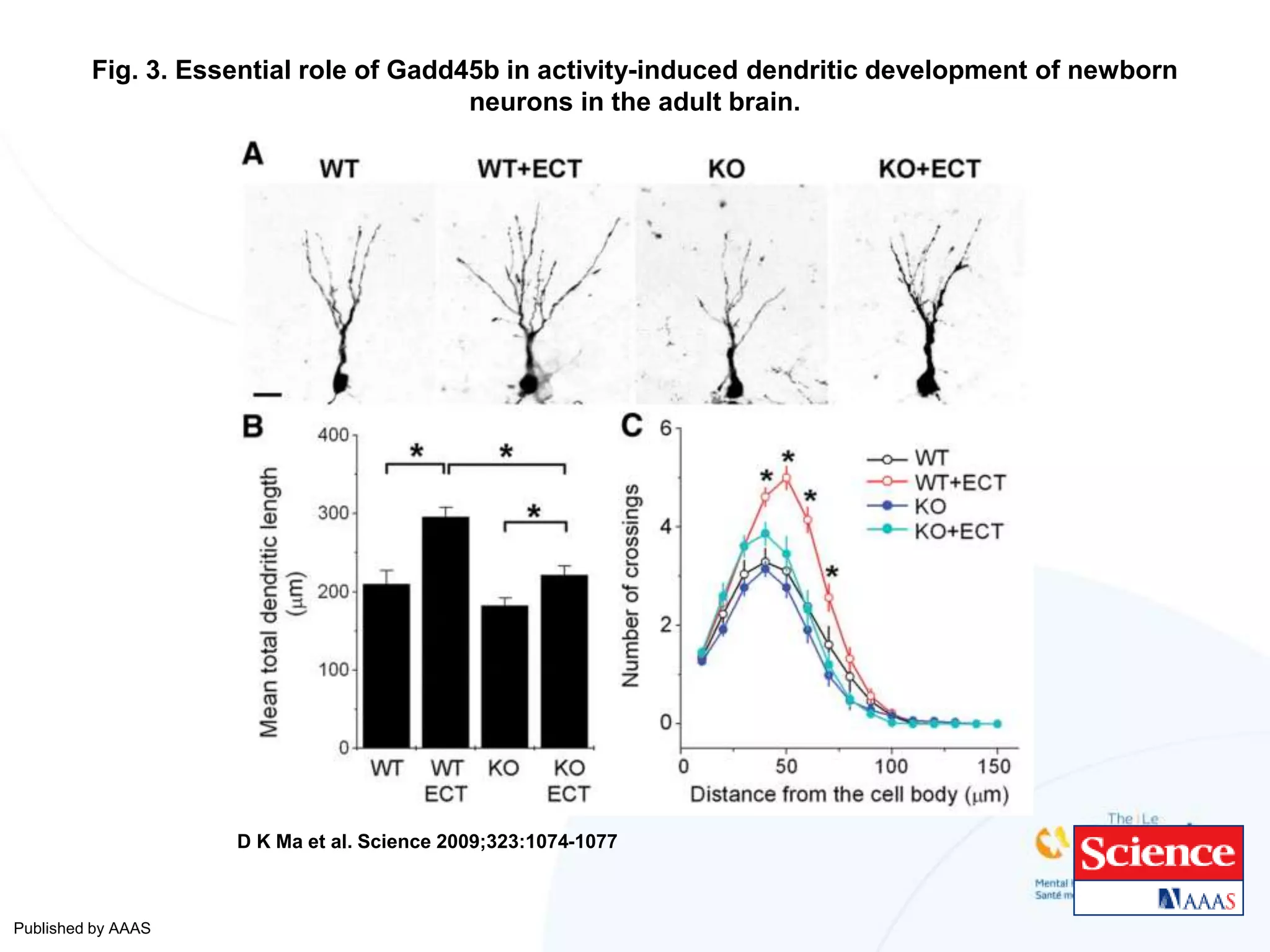
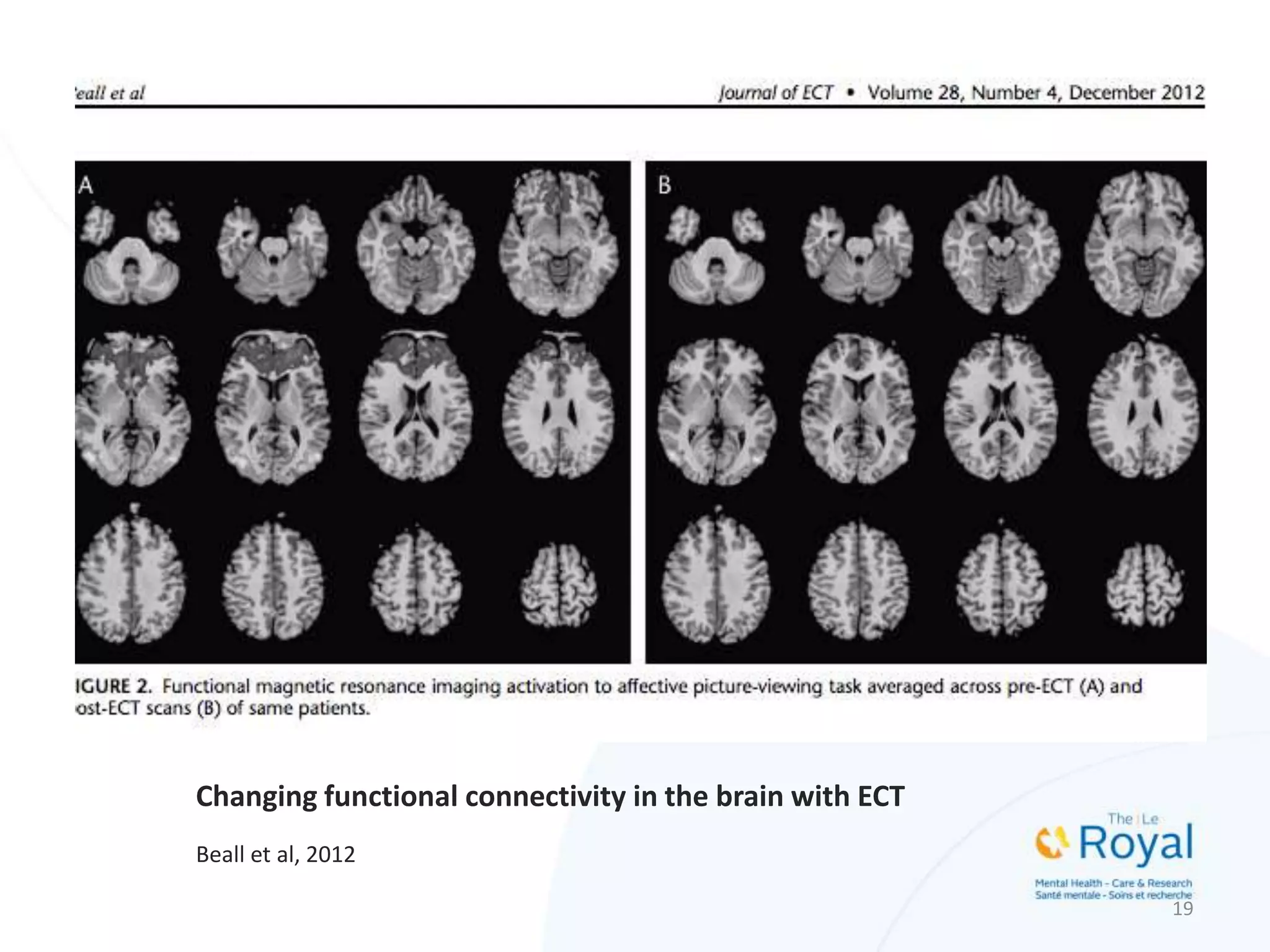

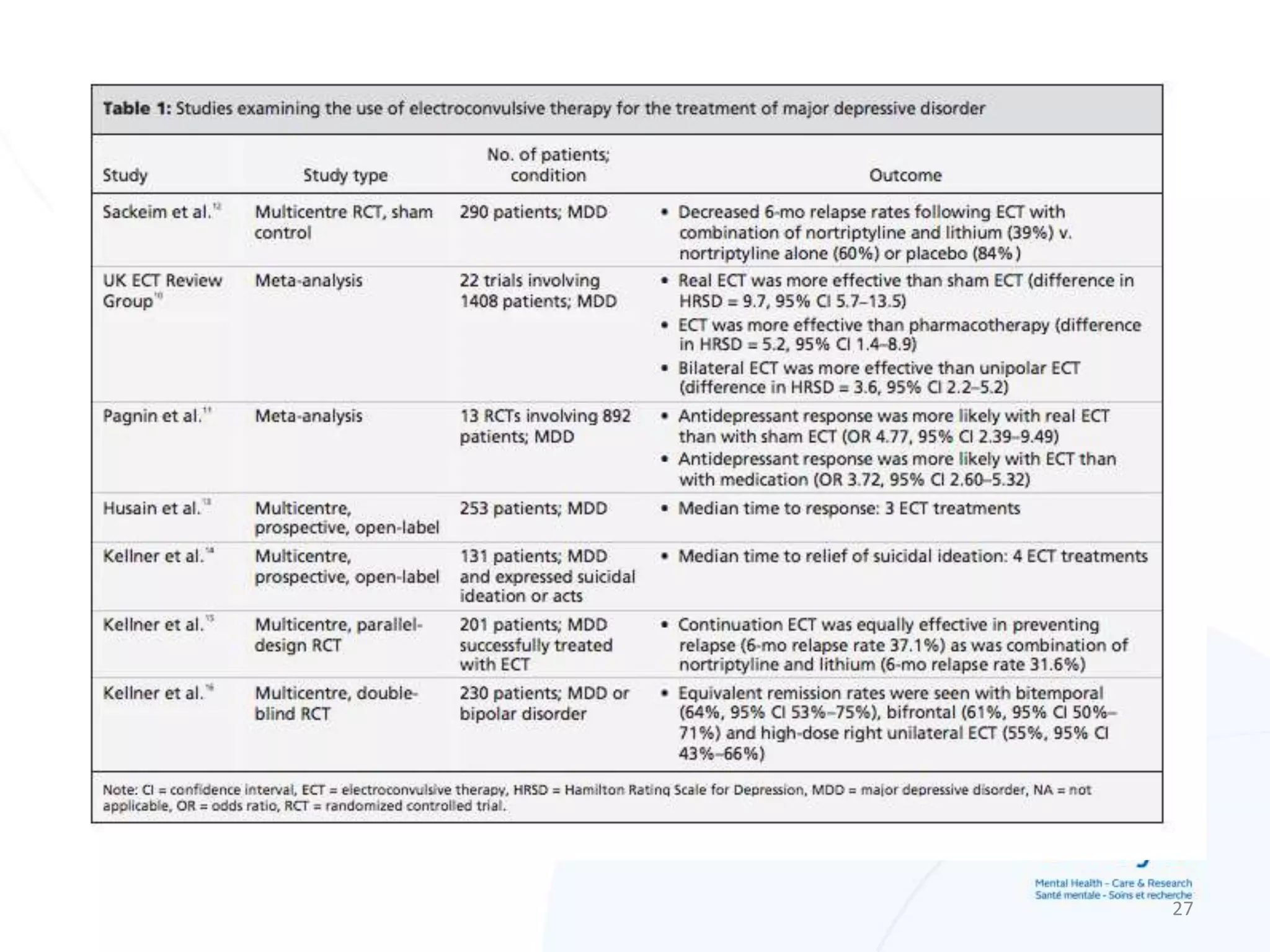








ECT, or electroconvulsive therapy, is a treatment that induces seizures in patients to provide therapeutic benefits for certain mental health conditions like severe depression. It works by altering neurotransmitter and receptor activity in brain regions involved in mood regulation. While its use declined due to negative portrayals, ECT is considered very effective and safe for treating conditions like major depression when other options have failed or cannot be tolerated. Common side effects include temporary memory loss that usually improves after treatment ends. Informed consent discussing risks, benefits, and alternatives is important given the cognitive effects.


























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
















