Downloaded 720 times


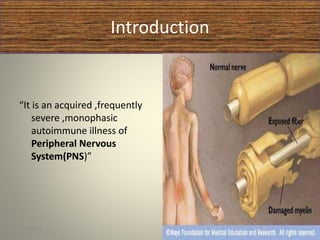






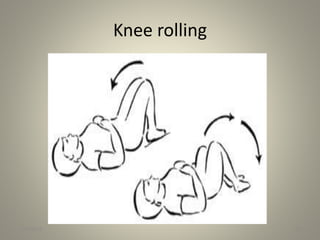
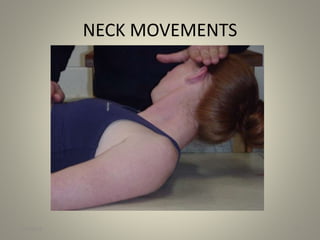
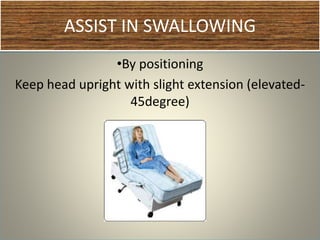
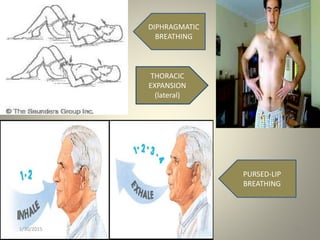






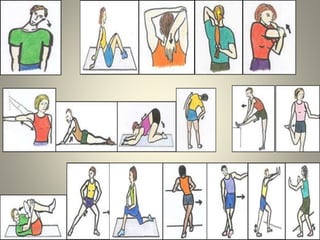


Guillain-Barré syndrome (GBS) is an acquired autoimmune disorder that causes inflammation of the peripheral nervous system. It can cause muscle weakness or paralysis. Physiotherapy management focuses on preventing complications like respiratory issues, contractures, and deep vein thrombosis during the acute phase. In subsequent phases, treatment includes stretching, strengthening, aerobic exercise, and balance training to aid recovery. Speech therapy may also be used to address swallowing difficulties that can occur with GBS.























































































