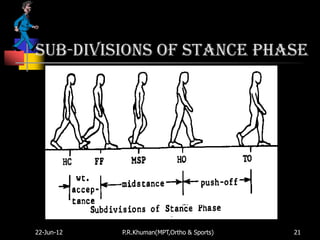
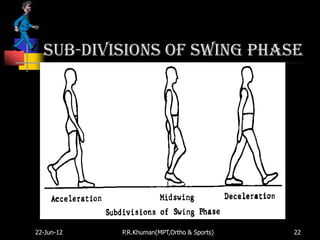
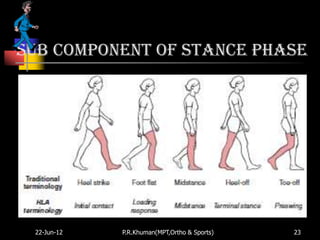
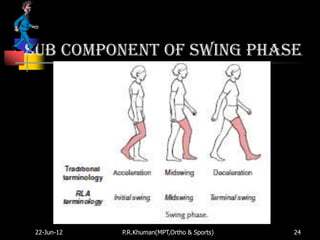
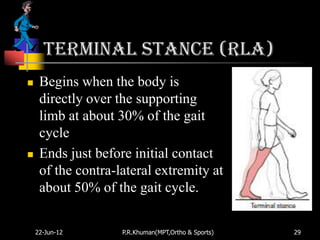
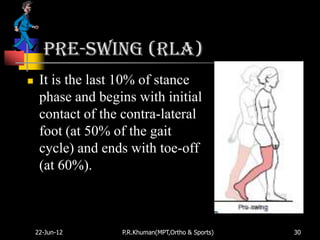
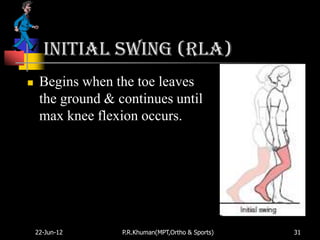
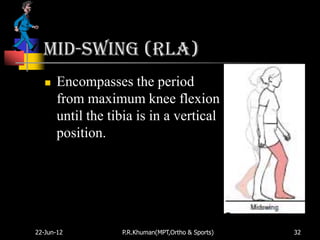
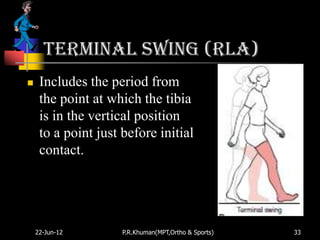
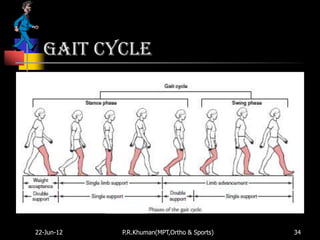
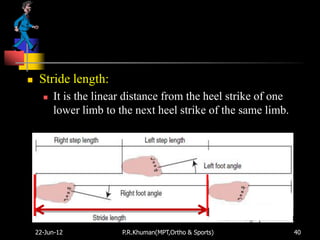
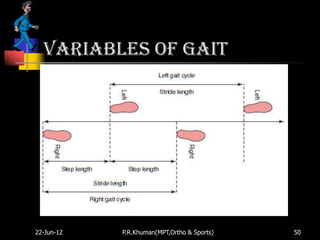
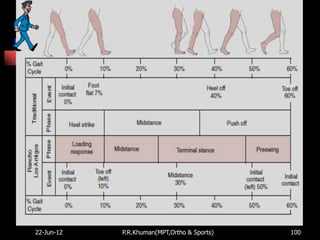
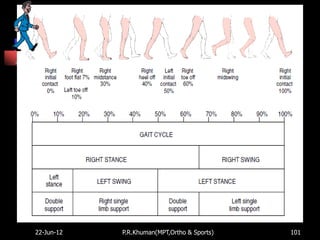
The document discusses normal and abnormal human gait. It defines gait as locomotion produced by coordinated movements of the body segments. The phases and components of the gait cycle are described in detail, including stance, swing, initial contact, loading response, mid-stance, terminal stance, pre-swing, initial swing, mid-swing and terminal swing. Temporal and distance variables that characterize gait are also outlined, such as stance time, single limb support time, double support time, stride length and step length. Factors that can influence gait variables are age, gender, height, joint mobility and muscle strength.

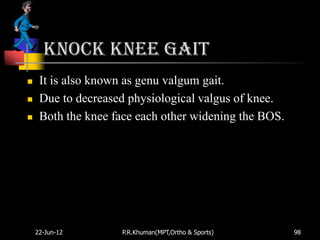
![Types of pathological gait
Due to pain –
Antalgic or limping gait – (Psoatic Gait)
Due to neurological disturbance –
Muscular paralysis – both
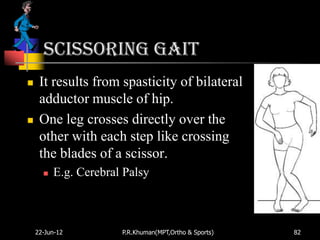
Spastic (Circumductory Gait, Scissoring Gait, Dragging or
Paralytic Gait, Robotic Gait[Quadriplegic]) and
Flaccid (Lurching Gait, Waddaling Gait, Gluteus Maximus
Gait, Quadriceps Gait, Foot Drop or Stapping Gait,)
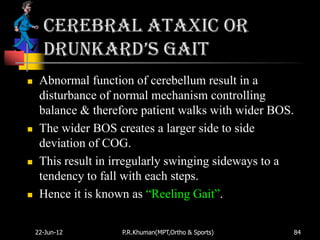
Cerebellar dysfunction (Ataxic Gait)
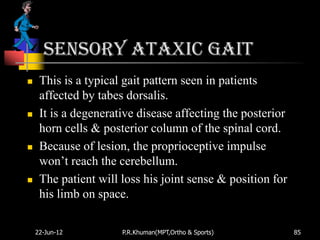
Loss of kinesthetic sensation (Stamping Gait)
Basal ganglia dysfunction (FestinautGait)
22-Jun-12 P.R.Khuman(MPT,Ortho & Sports) 68](https://image.slidesharecdn.com/gait-normalabnormal-120622041834-phpapp02/85/Gait-normal-abnormal-68-320.jpg)



























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















