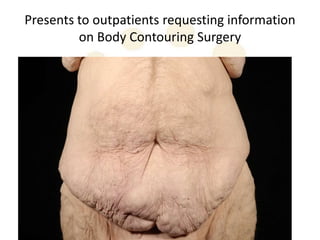
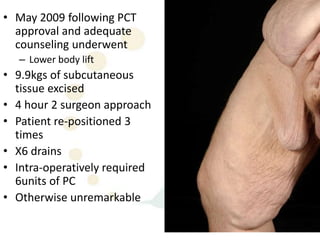
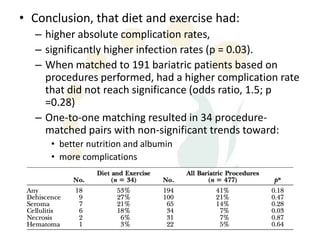
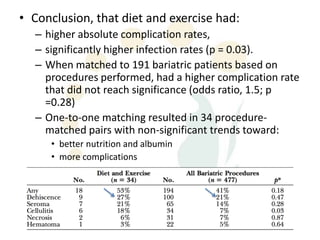
A 48-year-old man who lost 200 kg through diet and exercise underwent a lower body lift. During the 4-hour, 2-surgeon procedure, he required repositioning 3 times and 6 drains. Post-operatively he developed hemorrhages requiring exploration. He was discharged after 8 days requiring weekly drainage of seromas. The document discusses nutritional deficiencies common after bariatric surgery that can impact wound healing for body contouring procedures. It notes diet and exercise patients have higher complication rates than those who had bariatric surgery. Careful patient evaluation and counseling is important due to the risks and limitations of massive weight loss body contouring.