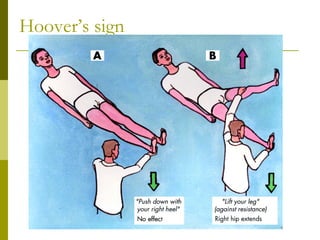
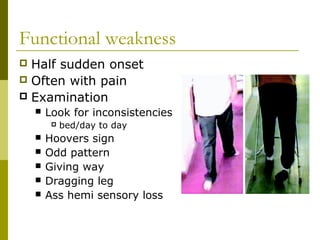
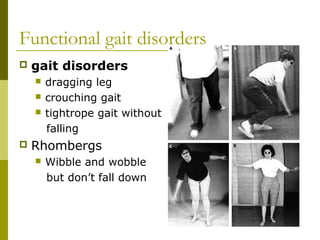
Functional neurology refers to neurological symptoms that are considered "functional" rather than due to identifiable organic disease. Two case studies are presented: a 16-year old girl with functional weakness and jerking movements, and a 34-year old woman with a sudden onset tremor. Investigations for functional disorders are typically minimal, while management involves explanation, psychiatry/psychology support like CBT, antidepressants, physiotherapy, and self-help resources. Prognosis is generally good, especially with early acceptance, short history, lack of other symptoms, and a supportive environment. The aims are to provide a swift diagnosis, consistent messaging to limit second opinions, and appropriate physical and psychological therapies.






































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






