Overview
Aim
The session willalso introduce the
special features of neurological history
taking and examination and the
language of neurology.
Learning outcomes
Describe the special features of the
neurological history and examination
Define some neurological terms
4.
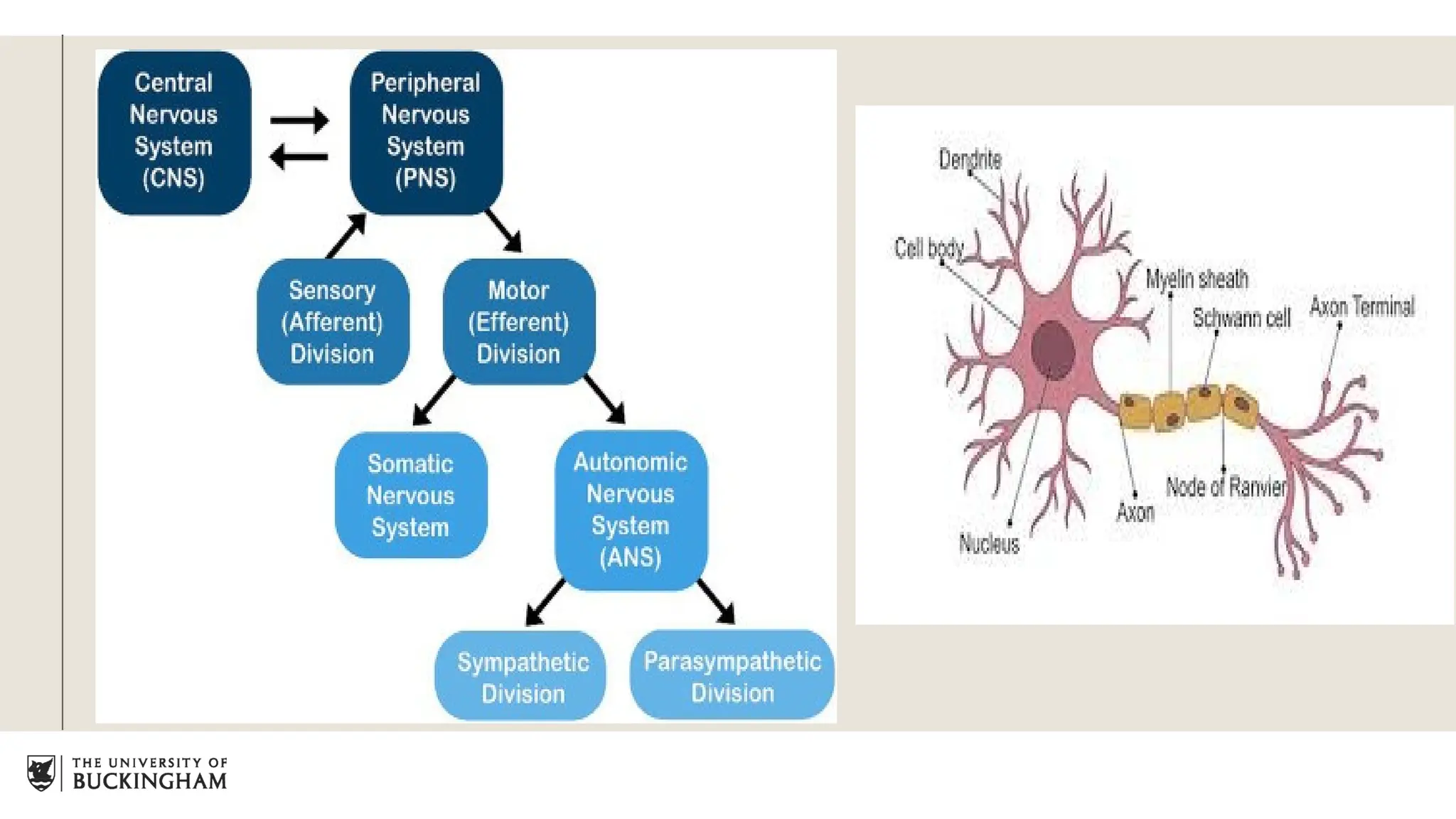
Neurons are thebuilding blocks.
Astrocytes provide structural framework whereas microglial cells are concerned with immune
and scavenging functions.
CNS- oligodendrocytes produces myelin sheath
PNS- Schwann cells produce myelin sheath.
Volume of CSF is around 140-270 ml which is replenished 3 to 4 times in a day with
production rate of 700mL/day.
Spinal cord contains afferent and efferent pathways which are responsible for motor and
sensory information transmission.
Sensory cell bodies of peripheral nerves are in the dorsal root ganglion.
Motor cell bodies are located in the anterior horn of the spinal cord.
General introduction
5.
History
TIME RELATIONSHIP
Forcommon neurological symptoms such as
headaches, numbness, loss of consciousness,
history is the key to diagnosis.
ALWAYS THINK WHERE IS THE LESION? WHAT
IS THE LESION?
Always remember to ask patients to define
symptoms in their own language.
O- onset(When did the symptom start?/when was he
well last time?)
(sudden, gradual/evolving)
D- duration(Persistent/intermittent)
P- progress ( Better or worse or same)
6.
What wasthe patient doing when the symptoms occurred?(Precipitating factor)
Anything which makes the patient's symptoms better or worse( time of the day, menstrual
cycles, posture or medications)(Relieving/exacerbating factors
Precipitating, exacerbating or relieving factors
7.
Associated
symptoms
With everydisease you have
associated symptoms like in
case of headache you will
have nausea, vomiting,
photophobia( aversion to
light) or
phonophobia( aversion to
sound)
8.
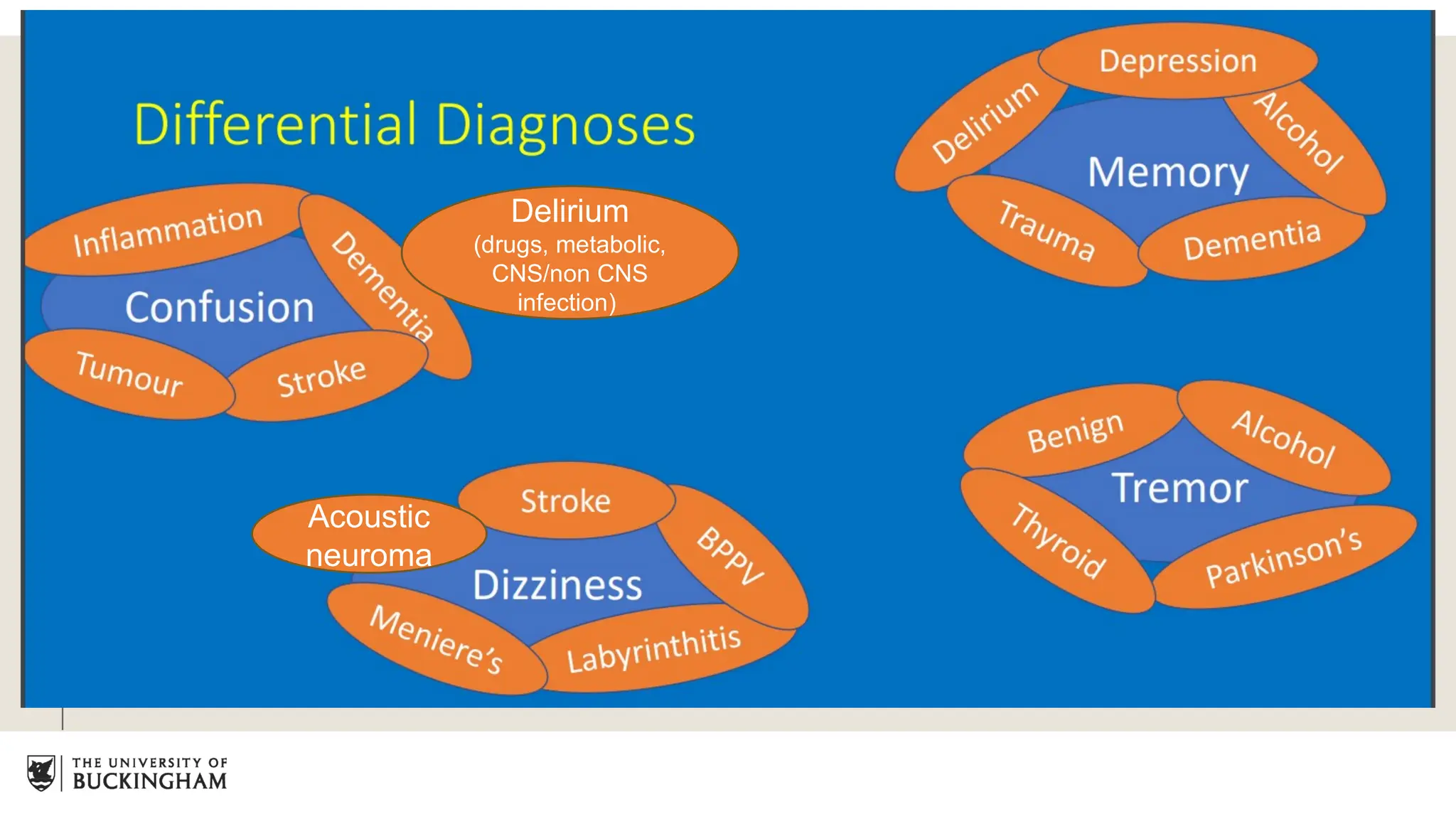
Presenting complaint inneurology
Common
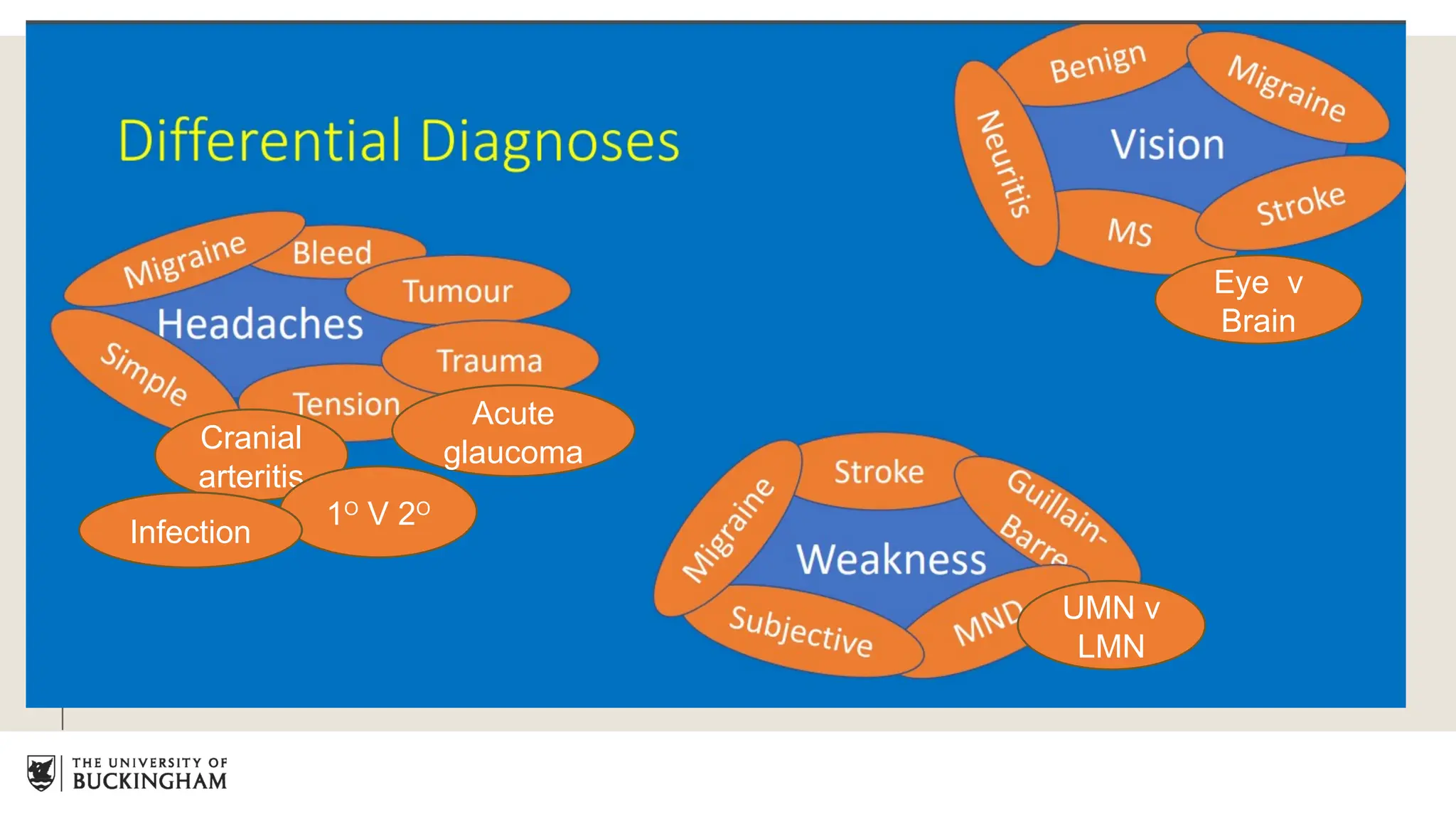
Headaches
Dizziness
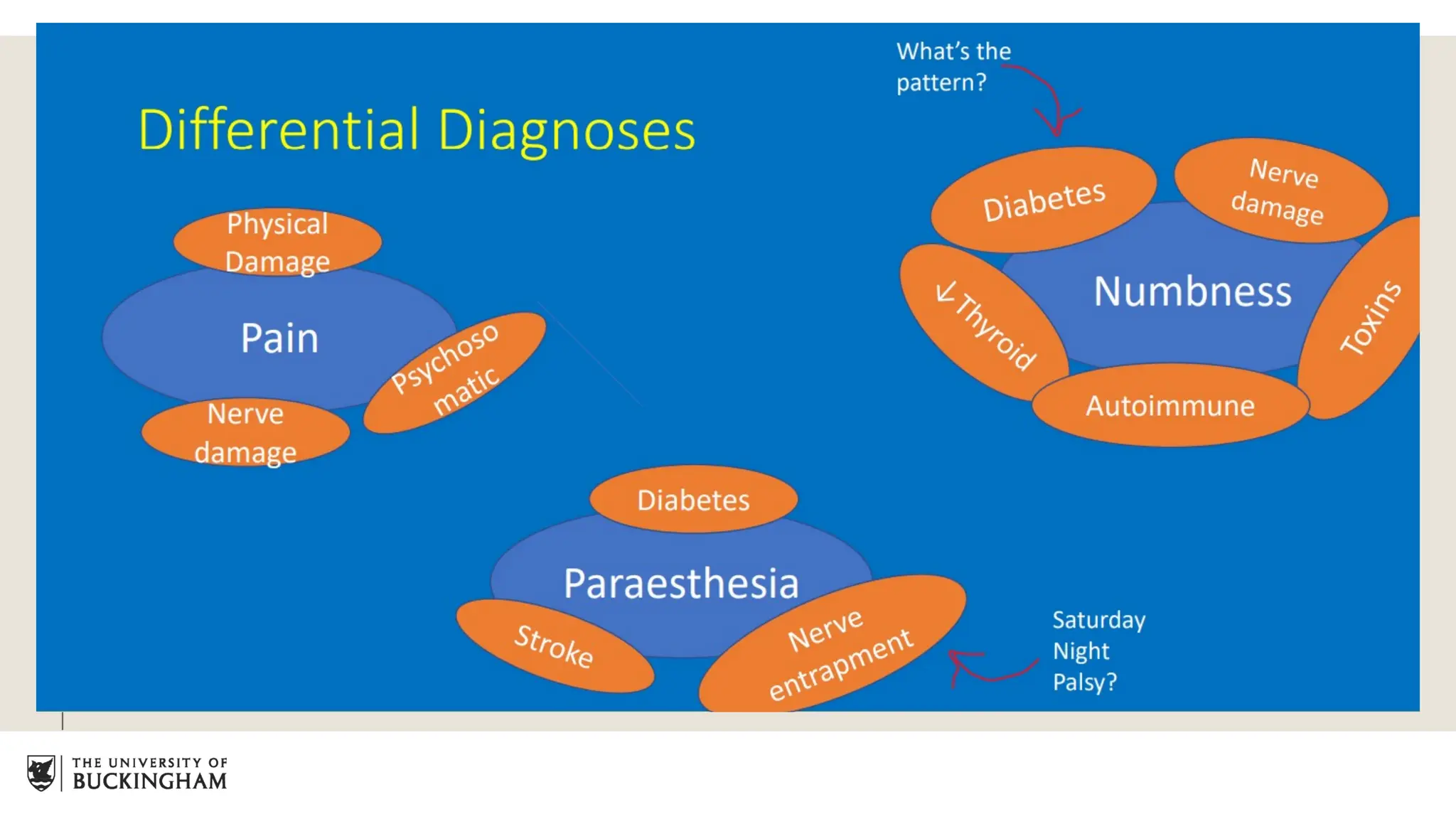
Pain
Numbness
Pins and needles
Weakness
Others
Memory
Shaking
Vision
Confusion
Loss of
consciousness
Questions
• Describe it to me?
• Frequency?
• Location?
• Precipitant, exacerbating/alleviating factors?
• RED FLAGS
• Thunderclap headache
• Slurred speech, weakness
• Incontinence of bladder/bowels
• Bilateral sciatica
• Seizures
• Acute confusion
• Fever
• Non blanching rash
9.
Other histories
PASTMEDICAL HISTORY- Symptoms which patients usually forget, birth history or
development history( in epilepsy), or hypertension, diabetes.
DRUG HISTORY- Prescribed, over the counters, complementary or recreational drugs.
FAMILY HISTORY- First degree relatives
SOCIAL HISTORY- Coping with the symptoms, affecting work?
Diet history especially vegetarians(VIT B12 intake), alcohol intake, drugs,
STDs, travel history
OCCUPATIONAL HISTORY- toxic peripheral neuropathy due to exposure any metals,
epilepsy for driving, cognitive levels for dementia.
10.
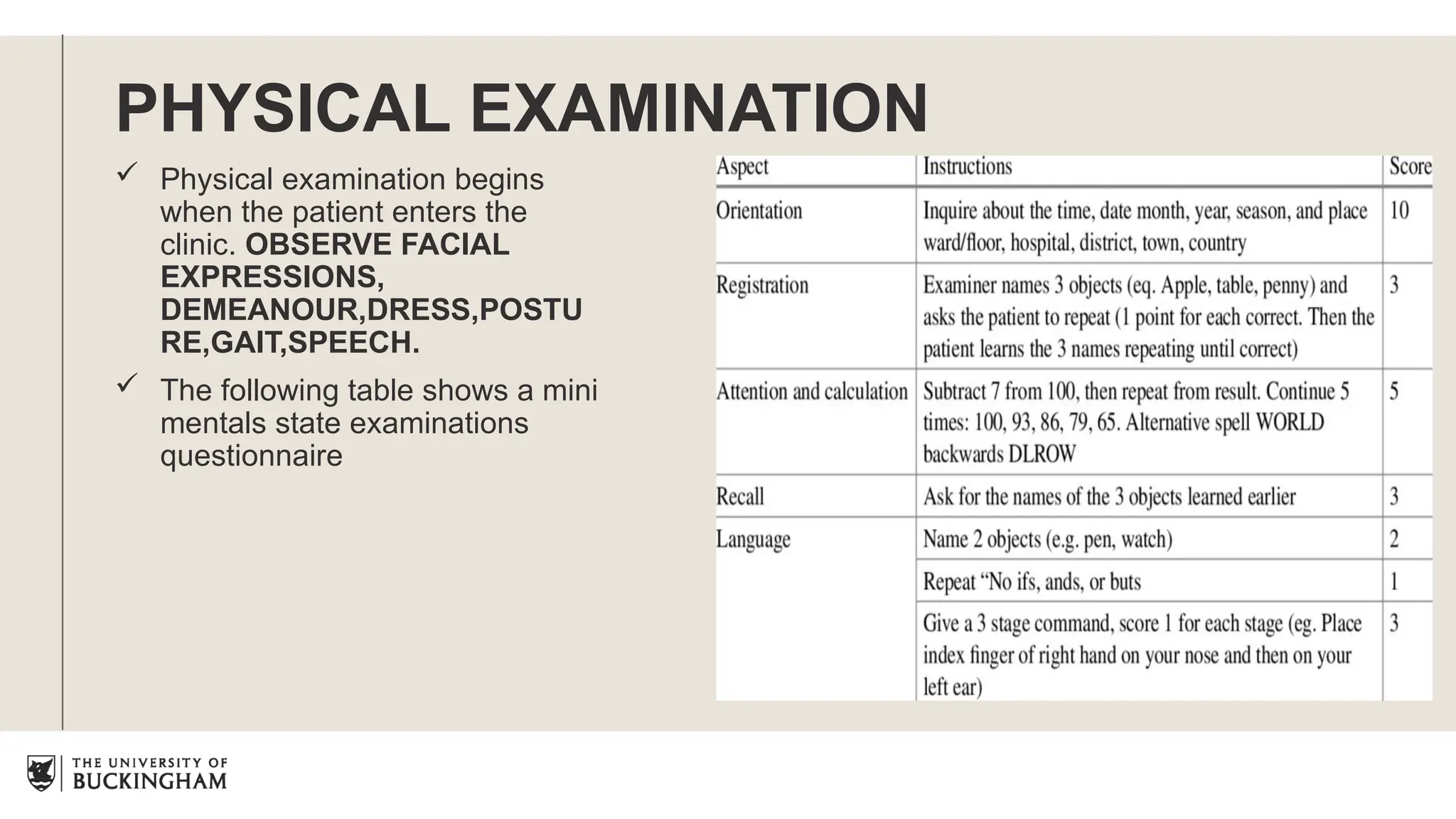
PHYSICAL EXAMINATION
Physicalexamination begins
when the patient enters the
clinic. OBSERVE FACIAL
EXPRESSIONS,
DEMEANOUR,DRESS,POSTU
RE,GAIT,SPEECH.
The following table shows a mini
mentals state examinations
questionnaire
12.
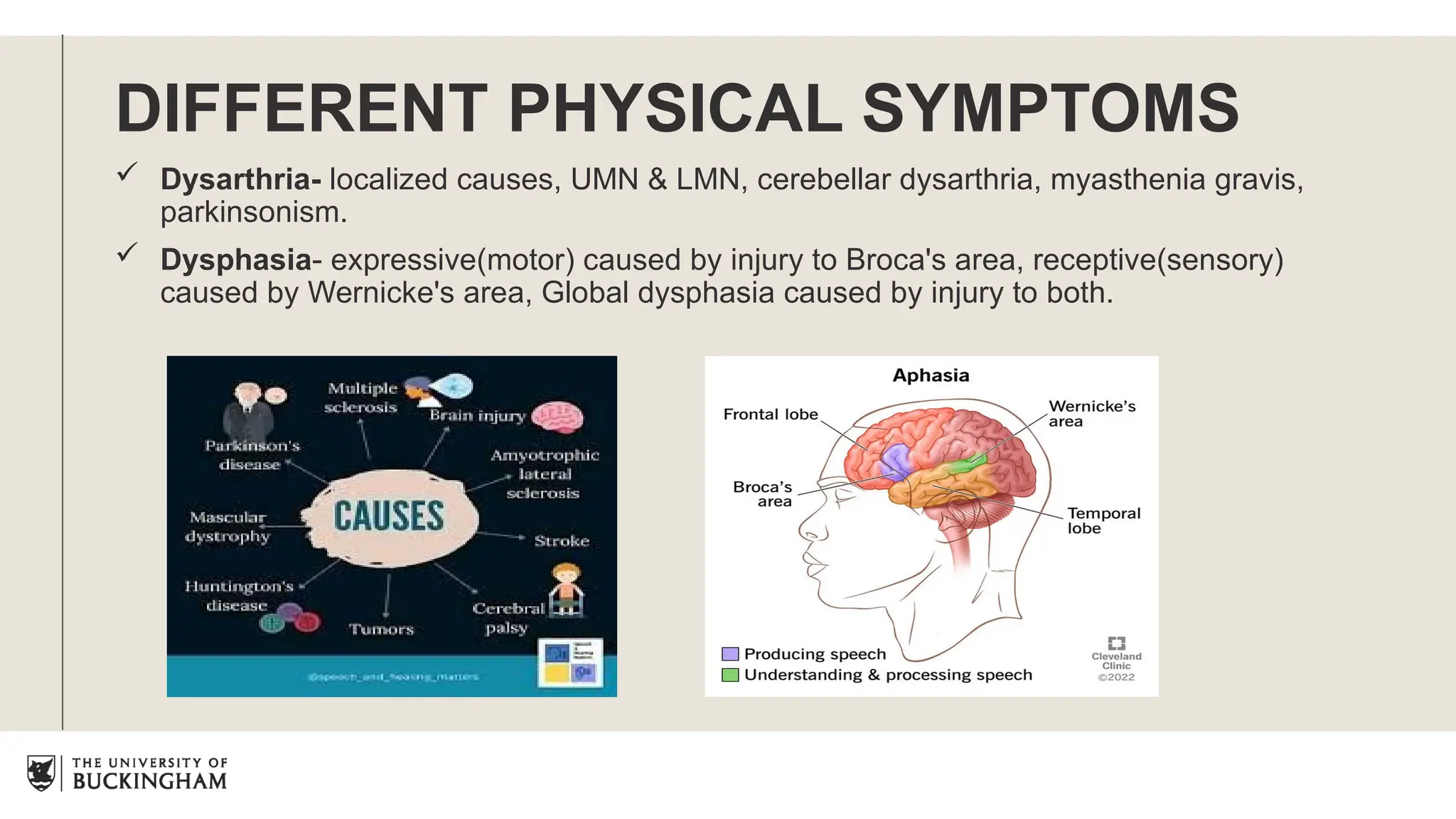
DIFFERENT PHYSICAL SYMPTOMS
Dysarthria- localized causes, UMN & LMN, cerebellar dysarthria, myasthenia gravis,
parkinsonism.
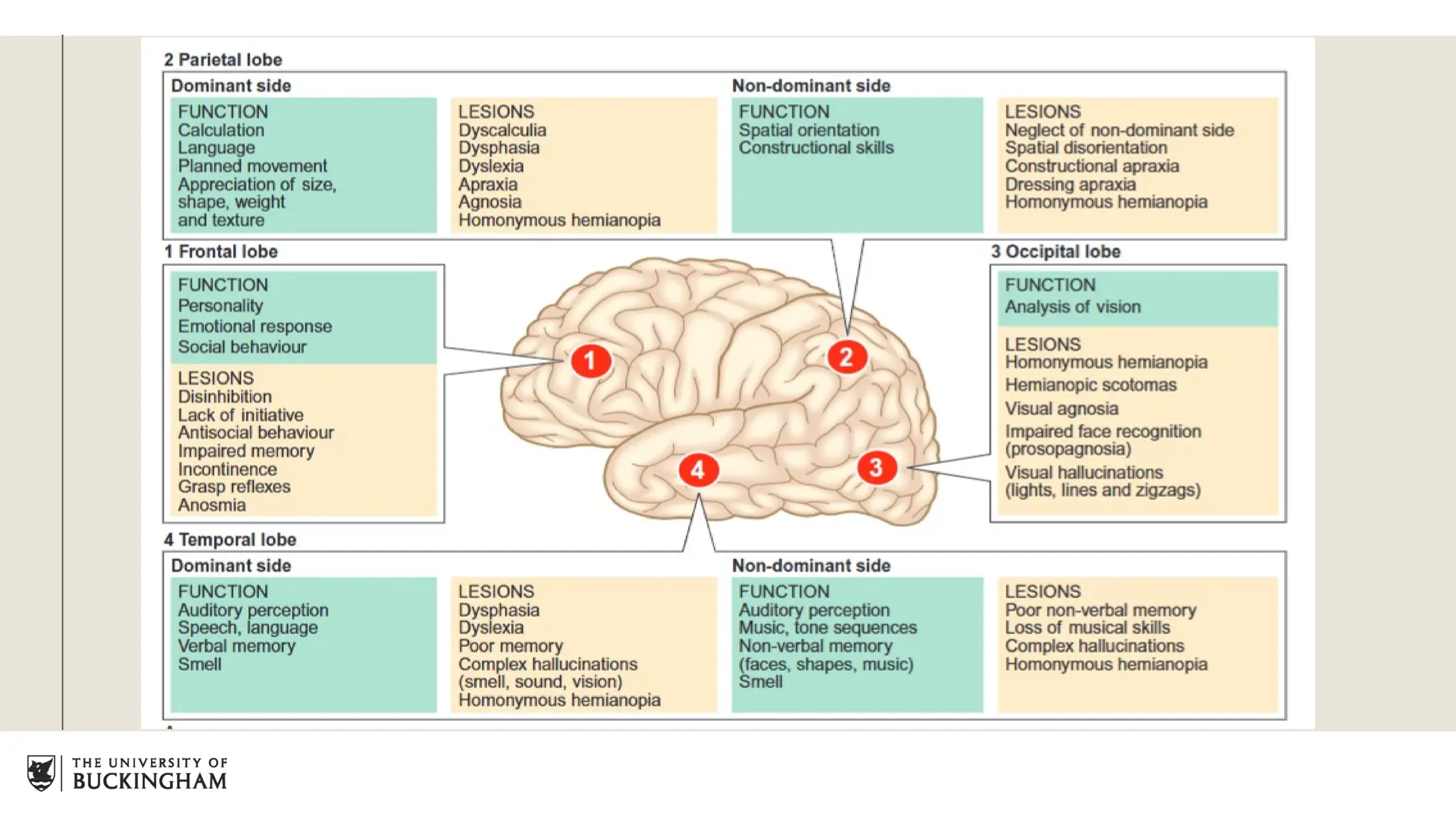
Dysphasia- expressive(motor) caused by injury to Broca's area, receptive(sensory)
caused by Wernicke's area, Global dysphasia caused by injury to both.
Assessment of motorsystem
Assessing CNS, PNS, basal ganglia, and cerebellar systems to test for motor
systems.
Assessment occurs in the following ways:
Stance & gait
Inspection & palpation of muscles
Assessment of tone
Testing of movement & power
Examination of reflexes
Testing of coordination
24.
Cerebellar examination
Dysdiadochokinesis
The inabilityto perform and sustain a series of repeated movements
Ataxia
Gross incoordination of movements – gait
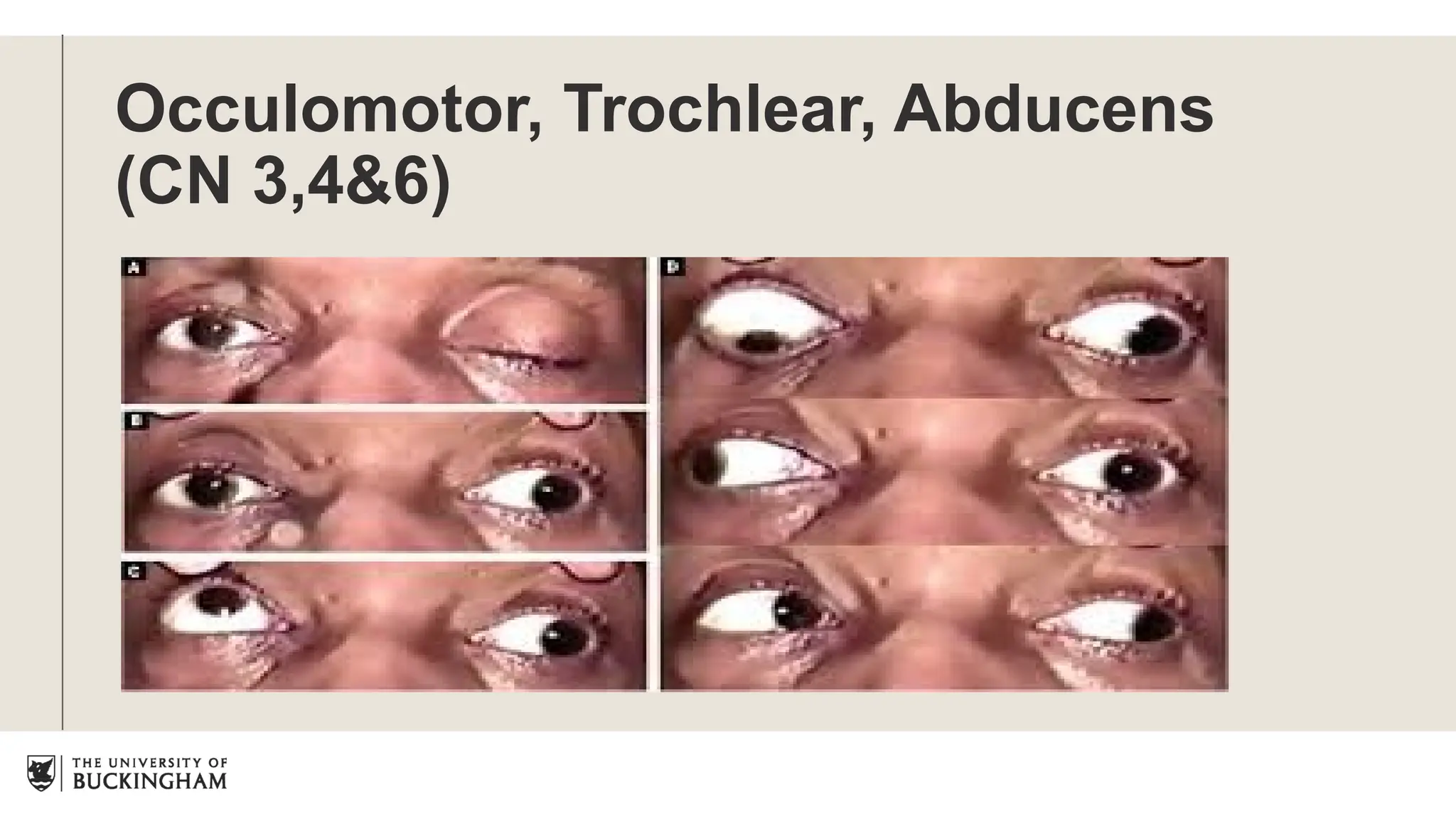
Nystagmus
Repetitive, involuntary oscillation of the eyes
Intention tremor
A wide tremor when performing voluntary movements
Slurred speech
Speech may be imprecise slow and distorted
Hypotonia
The patient may have muscle weakness
Pass pointing (dysmetria)
The patient overshoots when touching the examiners finger
25.
Stance & Gait
Stance(Standing) & gait (Walk)depends on intact visual, vestibular, sensory,
corticospinal, extrapyramidal along with functioning lower motor neurons and spinal
reflexes.
Unsteadiness on standing with eyes open suggests cerebellar ataxia.
Rhombergs test(Unsteadiness on standing with eyes closed ) suggests proprioceptive
sensory loss, bilateral vestibular loss.
28.
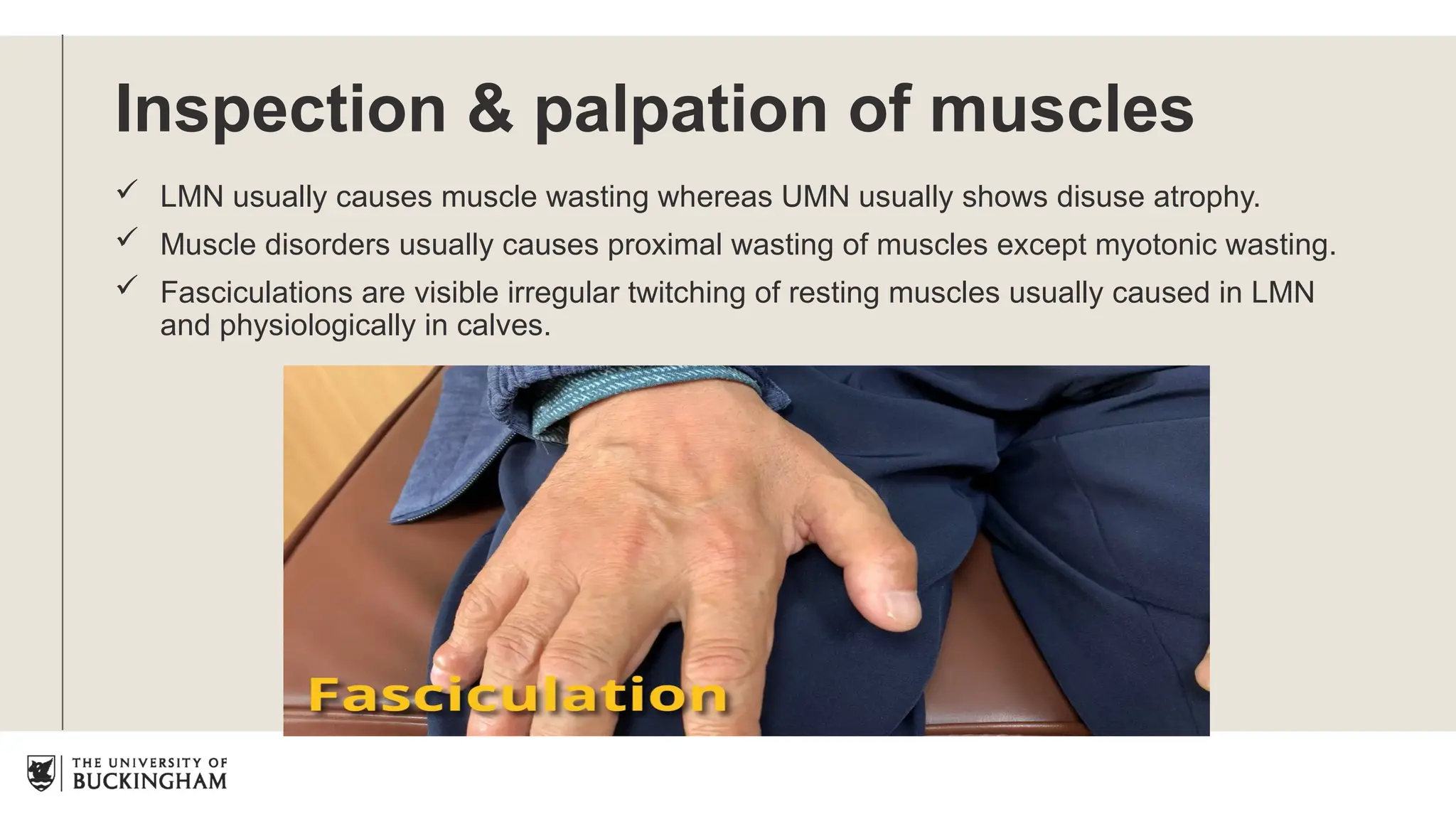
Inspection & palpationof muscles
LMN usually causes muscle wasting whereas UMN usually shows disuse atrophy.
Muscle disorders usually causes proximal wasting of muscles except myotonic wasting.
Fasciculations are visible irregular twitching of resting muscles usually caused in LMN
and physiologically in calves.
29.
Abnormal movements
Myoclonic jerks-sudden shock like contractions of one or more muscles that may be
focal or diffuse occur .singly or repeatedly. Pathologically seen in epilepsy, diffuse brain
damage and neurodegenerative disorders.
30.
Tremors
Tremor isan involuntary, oscillatory movement
about a joint or a group of joint resulting from
contraction and relaxation of muscles.
Physiological tremors are fine which can be also
seen in hyperthyroidism, excess alcohol or
caffeine intake
Parkinsonism causes pill rolling tremor
Isolated heat tremor caused in torticollis
Intention tremor usually seen in cerebellar
damage.
31.
Tone
Tone isthe resistance felt by the
examiner when moving a joint
passively.
Hypotonia is usually seen in LMN,
cerebellar disease, early phases of
cerebral or spinal shock.
Hypertonicity occurs in two forms:
spasticity and rigidity
Spasticity is velocity dependent
resistance to passive movements,
seen in UMN lesions.
Rigidity is sustained resistance
throughout the range of movement
and it is more easily detected when
the limb is moved slowly.
33.
Clonus
Clonus isrhythmic series of
contractions evoked by a sudden
stretch of muscle and tendon.
Unsustained clonus will be
physiological, but sustained denotes
UMN damage. Best seen in ankle
and knee
34.
Myotonia
It isdescribed as the inability of muscles to relax normally.
35.
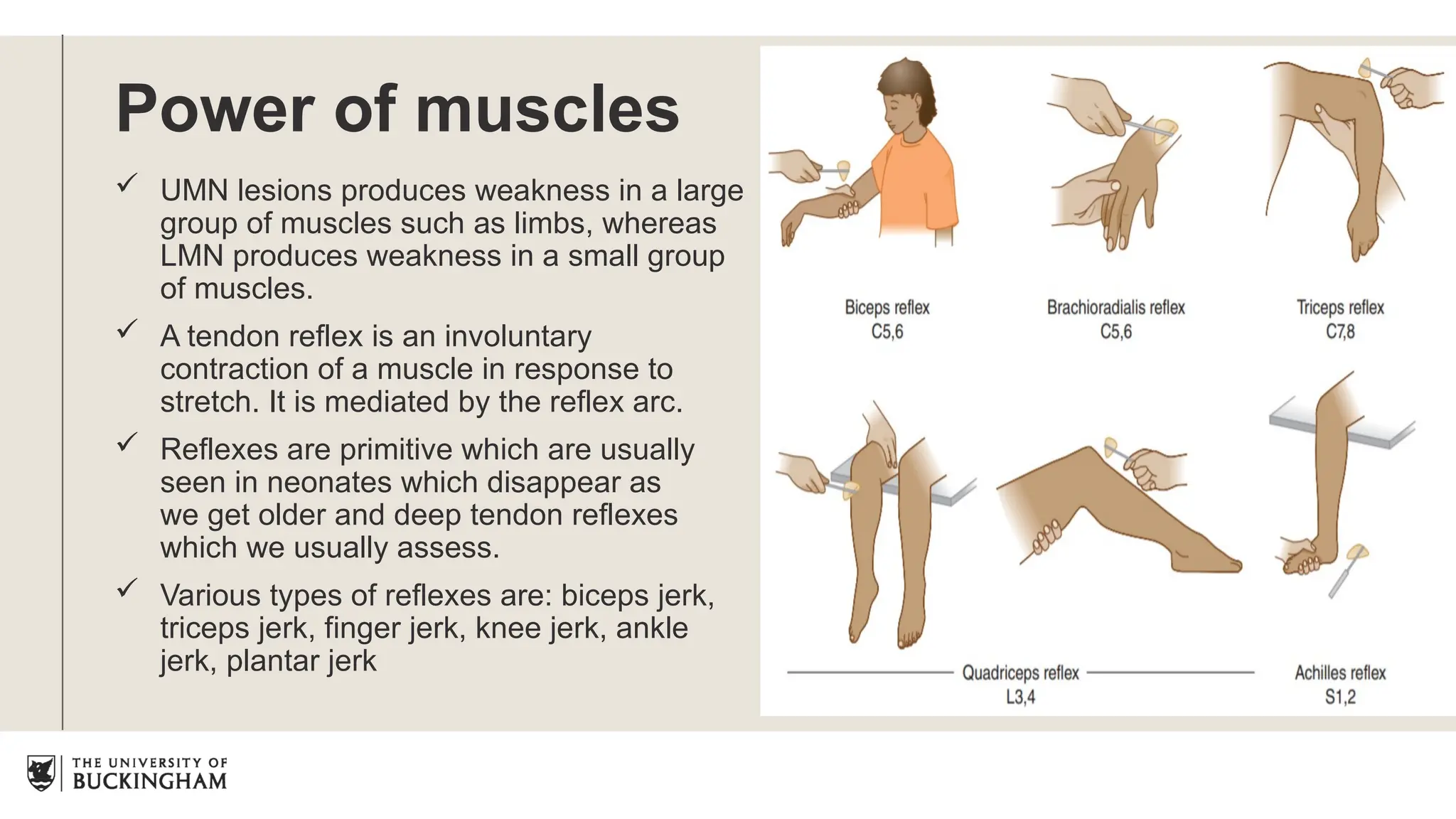
Power of muscles
UMN lesions produces weakness in a large
group of muscles such as limbs, whereas
LMN produces weakness in a small group
of muscles.
A tendon reflex is an involuntary
contraction of a muscle in response to
stretch. It is mediated by the reflex arc.
Reflexes are primitive which are usually
seen in neonates which disappear as
we get older and deep tendon reflexes
which we usually assess.
Various types of reflexes are: biceps jerk,
triceps jerk, finger jerk, knee jerk, ankle
jerk, plantar jerk
Apraxia
Apraxia/dyspraxia isdifficulty or inability to perform a task despite no sensory or motor
abnormalities. It usually denotes disturbance in higher cortical function in non-
dominant parietal or frontal lobe.
39.
Common presenting symptoms
Commonpresenting symptoms:
Paraesthesia: tingling, pins or needles.
Dysaesthesia: unpleasant paraesthesia
Hypoaesthesia: reduced sensation to normal sensation.
Analgesia: numbness or loss of sensation
Hyperaesthesia: increased sensitivity to stimulus.
Allodynia: painful sensation to a non- painful stimulus.
Hyperalgesia: increased sensitivity to a painful stimulus.
Investigations
Not necessary, do as and when required
Perform a basic blood test and then
perform a relevant imaging according to
the case.
Lumbar puncture – acute and
chronological conditions
Electroencephalography (EEG)- epilepsy,
encephalopathies or dementia &
Electromyography(EMG)- neurogenic and
myopathic pathologies
Nerve conduction studies- nerve
conductions and polyneuropathies
Mnemonic – VITAMINCDE
• V – Vascular
• I – Infective/Inflammatory
• T – Trauma/Toxins
• A - Autoimmune
• M – Metabolic
• I – Iatrogenic/Idiopathic
• N - Neoplastic
• C - Congenital
• D - Degenerative
• E - Endocrine
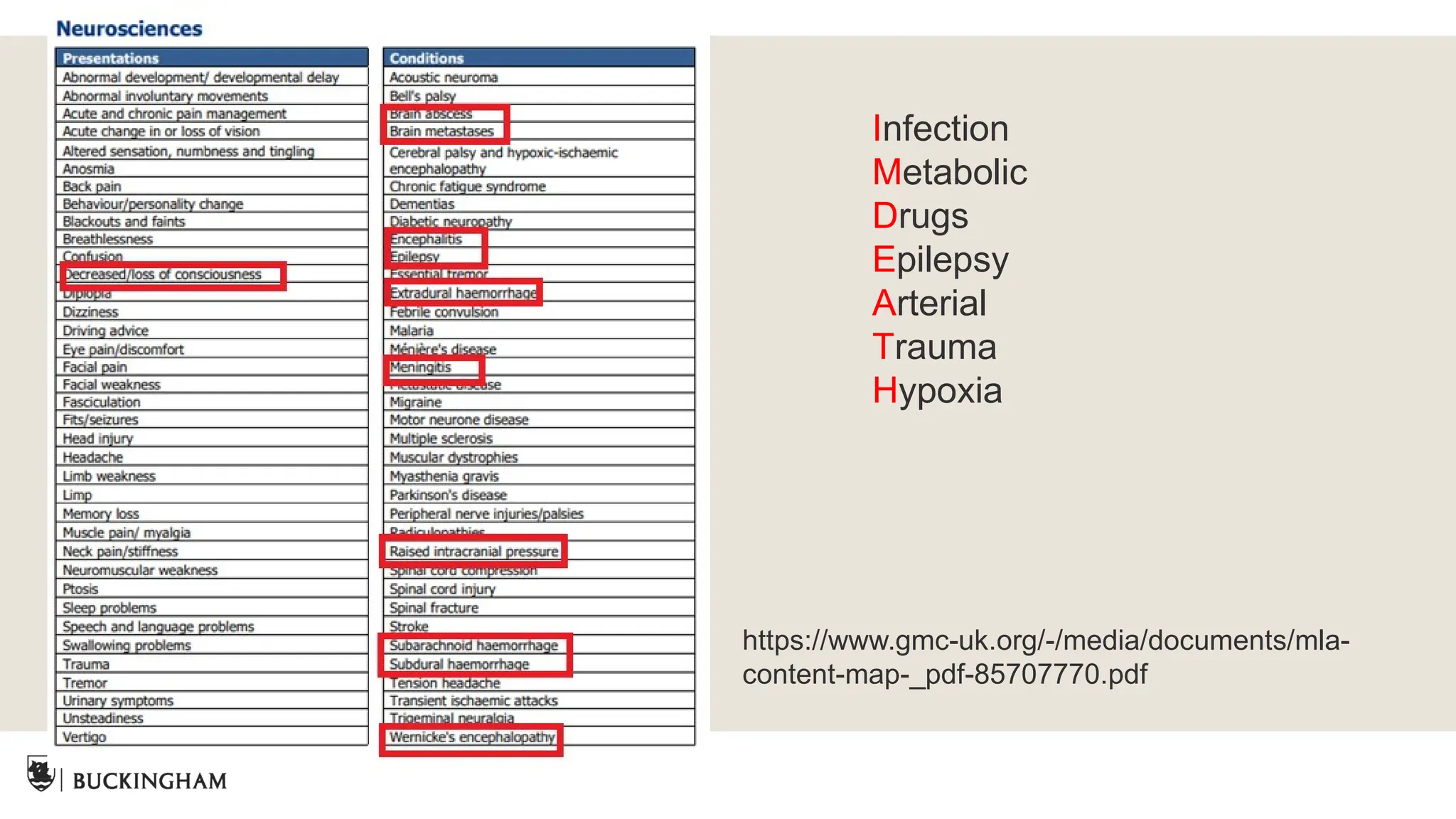
Differential Diagnoses
46.
Special tests
Pronator drift
Signof a contralateral UMN lesion
Rombergs test
Proprioception, vestibular function and vision
Normal test requires healthy functioning of the dorsal spinal columns
(proprioception)
Sciatic and femoral stress test
Tinnels/phalens tests
Test for carpal tunnel syndrome – median nerve compression
Swinging light test
Relative afferent pupillary defect (RAPD)
Detect dysfunction in retinal or optic nerve
Retinal detachment, optic nerve damage-raised ICP or MS






















![Central Nervstem notes [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/centralnervoussystemnotesautosaved-250325012003-ecd5223c-thumbnail.jpg?width=640&height=640&fit=bounds)

























