

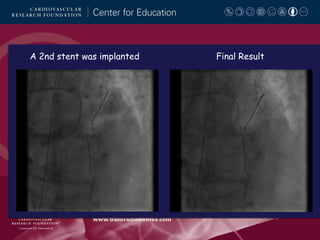
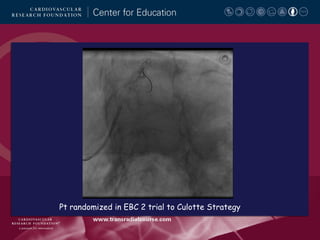
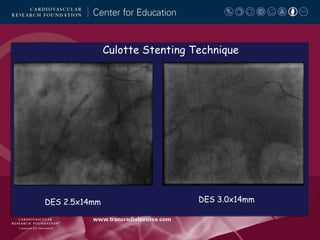
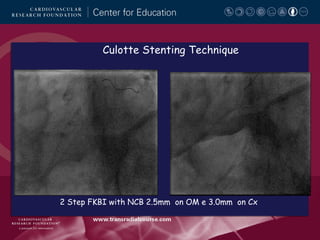
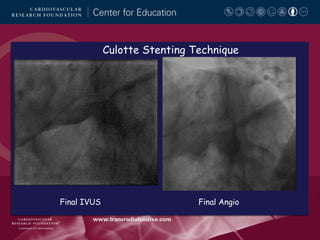
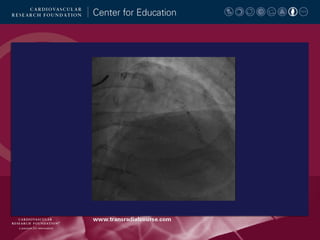
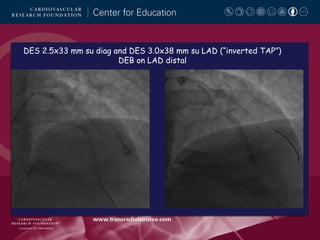
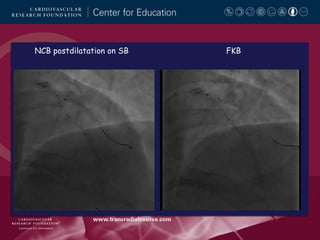
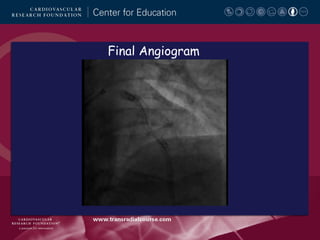
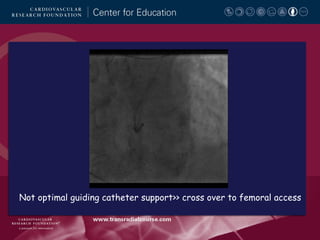
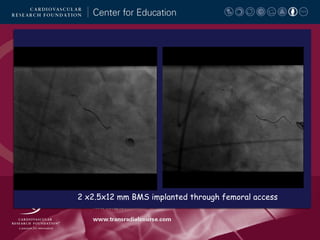
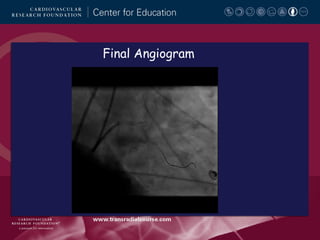
This document summarizes the techniques used at the presenter's center for treating bifurcation lesions through radial versus femoral access. It provides examples of bifurcation cases treated through radial access using provisional stenting or two-stent techniques. The conclusions state that most bifurcations can be treated through radial access but femoral access may be considered if backup support is suboptimal or simultaneous implantation of two stents is needed, such as for conventional mini-crush or V stenting.























































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















