Download to read offline



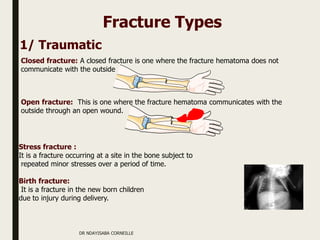





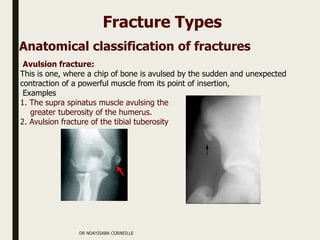













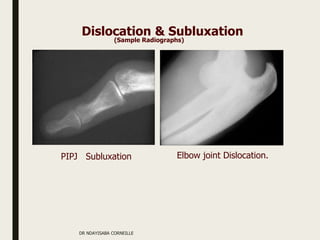



The document, presented by Dr. Ndayisaba Corneille, covers the definition and classification of fractures, dislocations, and subluxations, along with their causes, symptoms, and management principles. It elaborates on various types of fractures, their healing process, and potential complications, emphasizing the importance of radiography in diagnosis and treatment. Additionally, it outlines the essential steps for fracture management, including first aid, immobilization, and rehabilitation strategies.























































































