Download as PDF, PPTX
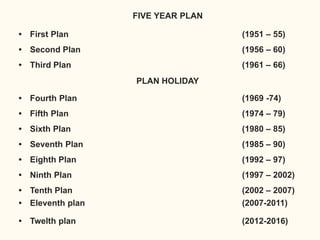
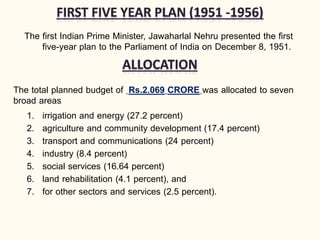
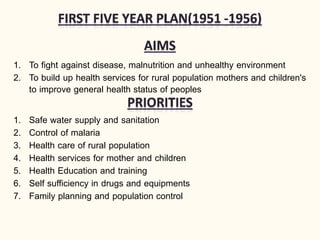
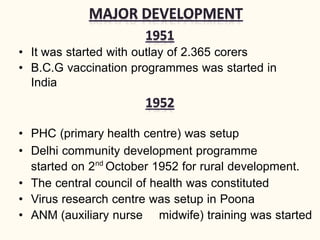






The document discusses India's five year plans with a focus on healthcare. It provides a history of the Planning Commission and outlines the objectives and functions of the first several five year plans from 1951-1990. The plans aimed to improve health services, control diseases, promote family planning and sanitation, and increase access to care especially for rural populations. Key initiatives included expanding primary health centers and immunization, and programs for malaria, smallpox, and family planning.





















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

