Download to read offline



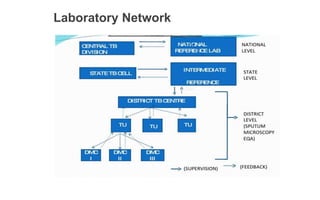
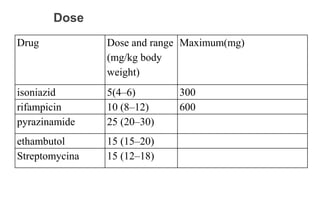



The document describes India's Revised National Tuberculosis Control Programme (RNTCP). It outlines the objectives, history, organization, and initiatives of the RNTCP. Key points include: the RNTCP adopted the internationally recommended DOTS strategy in 1993 to address low treatment success rates; its laboratory network includes national reference labs, intermediate reference labs, and microscopy centers; it treats TB using standard short course chemotherapy regimens; and new initiatives include the Nikshay case-based surveillance system and expanding rapid diagnostics and drug-resistant TB treatment. The national strategic plan for 2012-2017 aims for universal TB care access through early detection and treatment of 90% of cases.



































































