Downloaded 477 times

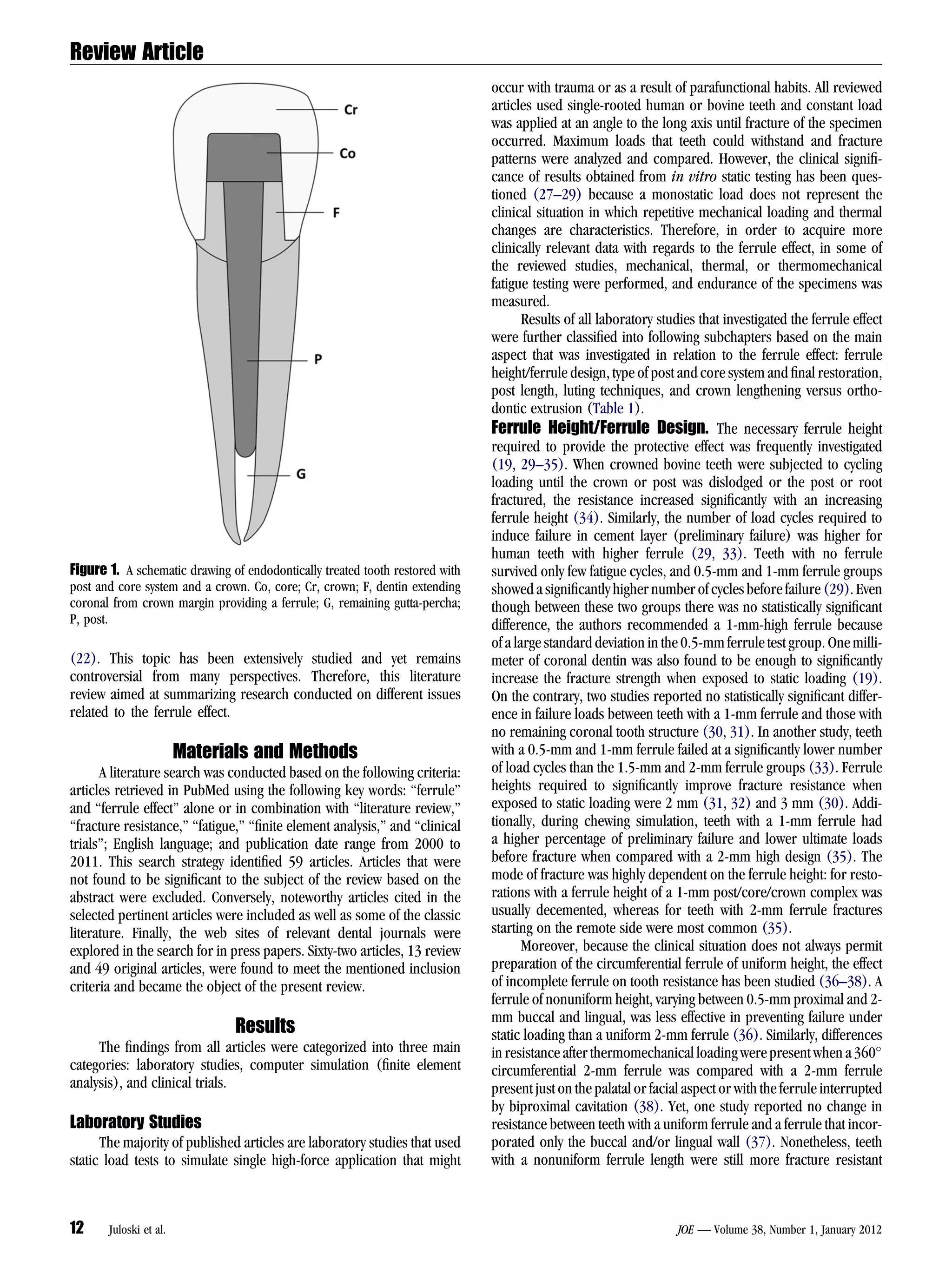




This literature review summarizes research on the ferrule effect, which refers to the protective effect provided by dental structure surrounding the tooth restoration. The main findings are: 1) Laboratory studies found that a ferrule height of 1.5-2 mm has a positive effect on fracture resistance, and an incomplete ferrule is better than no ferrule. 2) Computer simulations found that including a ferrule can lead to more favorable fracture patterns. 3) Clinical trials provided evidence that an adequate ferrule lowers the impact of other factors, like the post system, on tooth performance. When a ferrule cannot be provided, orthodontic extrusion is preferable to crown lengthen























































































