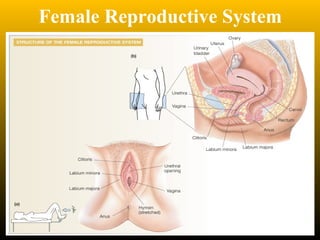
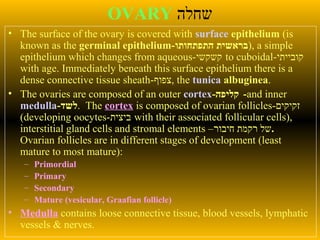
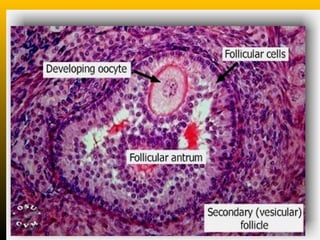
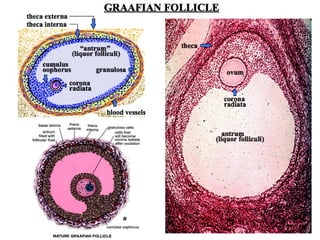
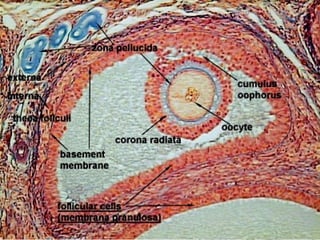
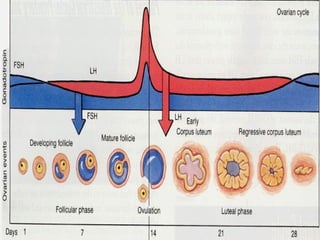
The document describes the key parts of the female reproductive system including internal organs like the ovaries, oviducts, uterus, and vagina as well as external genitalia. It provides details on the ovaries and ovarian follicles, discussing their development from primordial to secondary to graafian follicles. It explains ovulation, the formation and role of the corpus luteum, and the ovarian and hormonal cycles. Key points are summarized around follicular development and atresia, ovulation, the corpus luteum, and the oviduct's role in transporting the ovum and embryo.







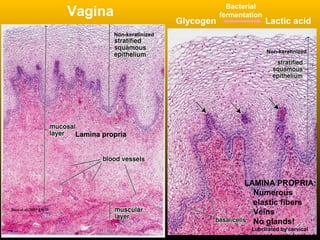
![Vagina
• The lamina propria contains many elastic fibers, a large
venous plexus and NO GLANDS.
• Lubrication is provided by the cervical glands and by the
vestibular mucous glands (present at the opening [vestibule]
of the vagina; a.k.a. Bartholin’s glands).
• The epithelial cells are continually desquamated and contain
much glycogen when estrogen levels are high (ovulation).
• Bacteria in the vagina ferment the glycogen to form lactic
acid, thus lowering the pH. The acidic environment inhibits
the growth of some pathogenic microorganisms.
• Post-menopausal women do not secrete much glycogen
because of their low estradiol levels; the subsequent higher
vaginal pH can lead to increased vaginal infections.](https://image.slidesharecdn.com/female2007i-140519080135-phpapp02/85/Female-Histology-94-320.jpg)





















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









