Downloaded 54 times

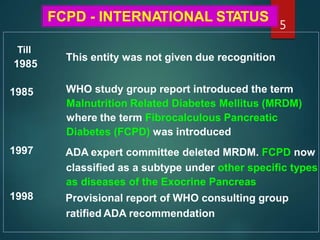
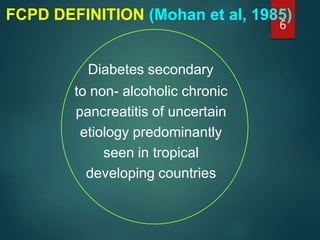


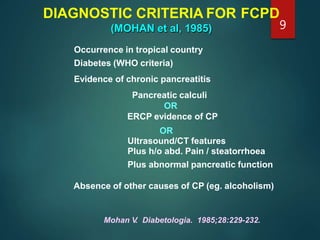
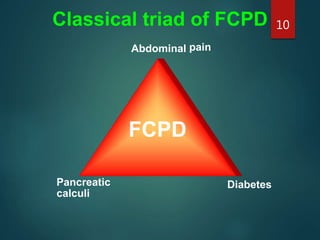
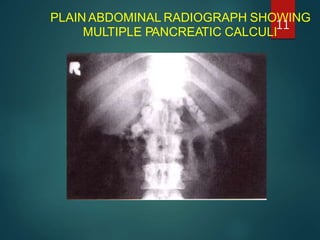
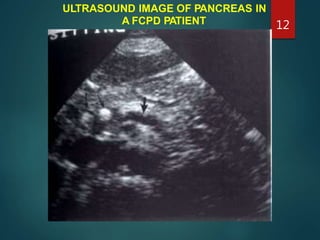
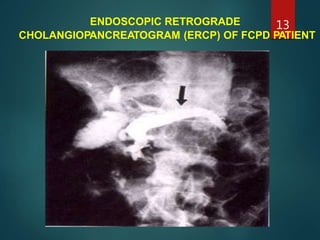
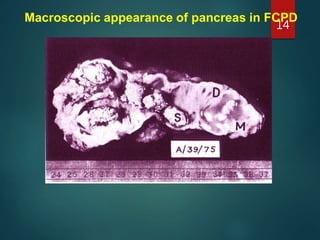
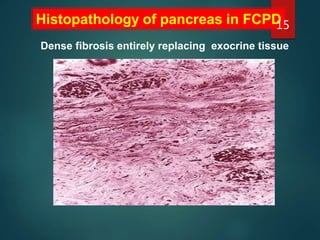
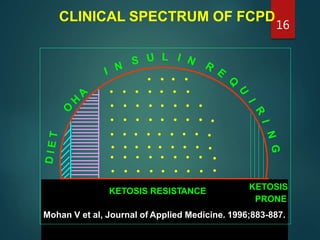
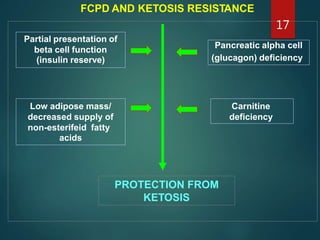
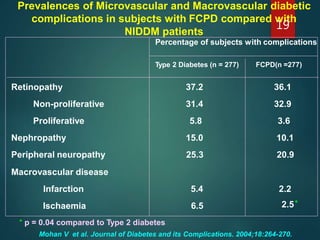
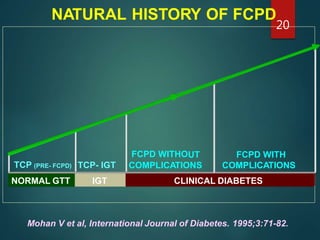

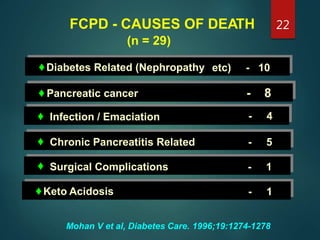

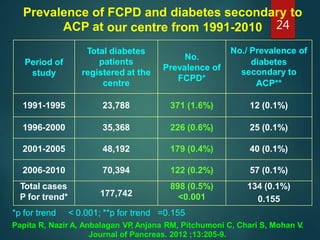
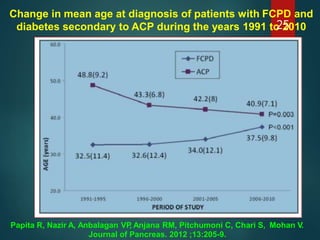
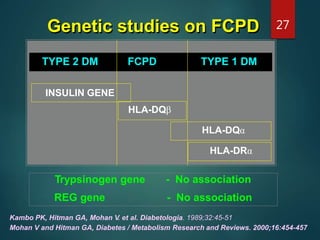
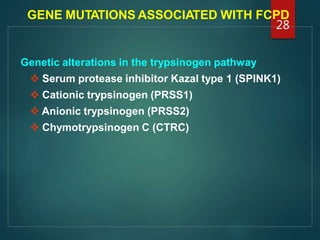
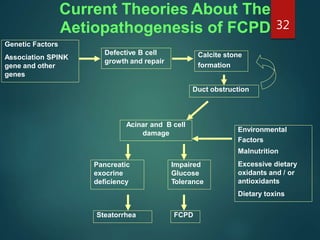

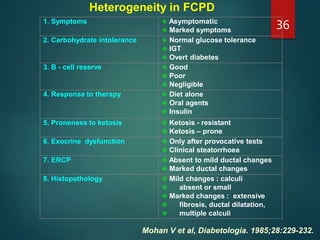

This document provides information about Fibrocalculous Pancreatic Diabetes (FCPD). It discusses the historical background and definitions of FCPD. FCPD is characterized by severe diabetes associated with chronic pancreatitis and pancreatic stones. It predominantly affects poor populations in tropical developing countries. The document outlines the diagnostic criteria and clinical manifestations of FCPD. It also discusses the genetic factors, various theories about the etiopathogenesis, and principles of management including treatment of diabetes and abdominal pain. FCPD shows heterogeneity in its presentation and natural history.