Download to read offline

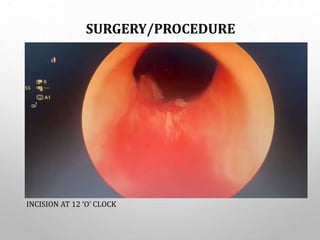
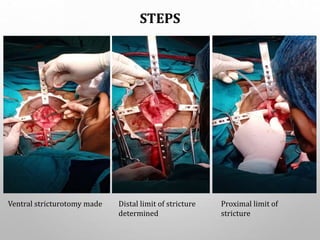
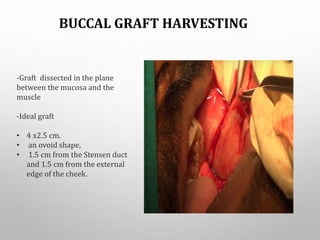
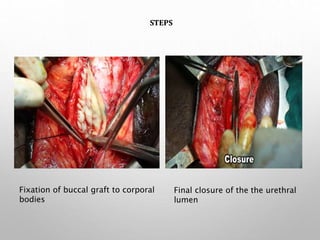
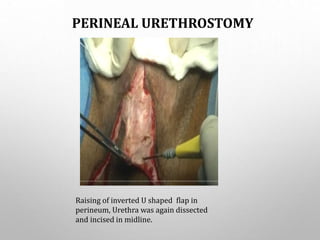

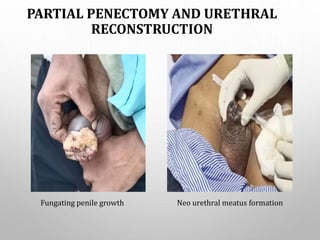

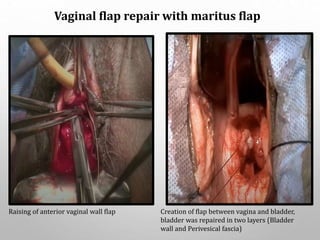
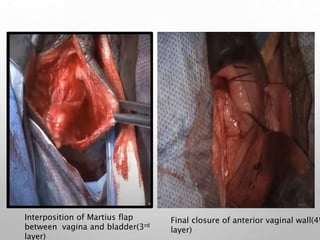
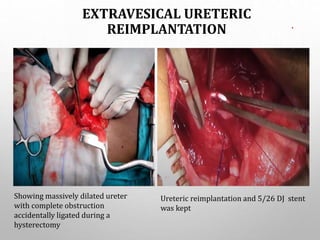

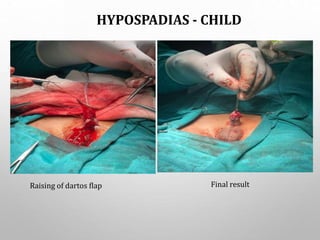


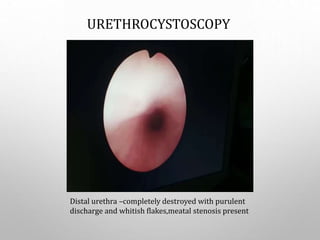
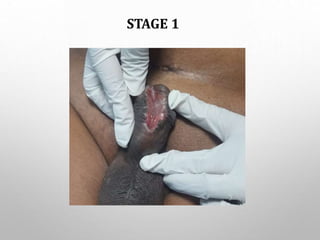
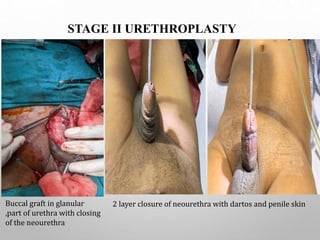


This document provides case summaries of various urological procedures performed by Dr. Amit Kumar Mishra at AIIMS Raebareli. The procedures included direct visual internal urethrotomy for urethral stricture, buccal mucosal graft urethroplasty, perineal urethrostomy, partial penectomy with urethral reconstruction, vaginal flap repair of urethrovaginal fistula, extravesical ureteric reimplantation, Jordan's flap procedure for urethral stricture, hypospadias repair in children and adults, staged urethroplasty, transurethral resection of bladder tumor, and transure






















































