Downloaded 10 times



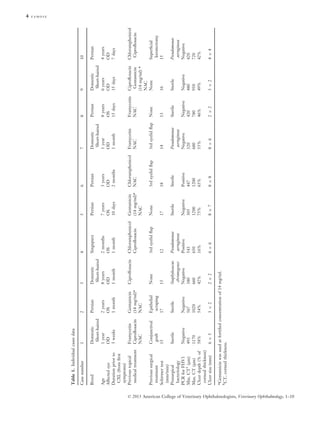

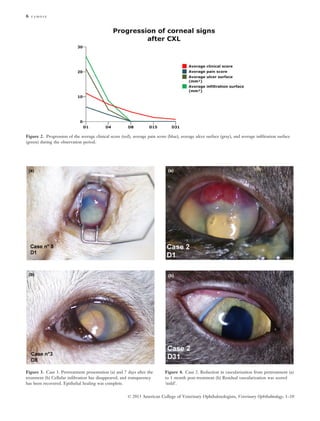





This study evaluates the effectiveness of accelerated collagen cross-linking (CXL) for treating melting keratitis in ten cats. The results indicated significant pain relief, epithelial healing, and resolution of cellular infiltration by day 8, with all cases maintaining visual function at 30 days post-treatment. Overall, accelerated CXL emerged as a promising option for managing this serious ocular condition in felines.























































































