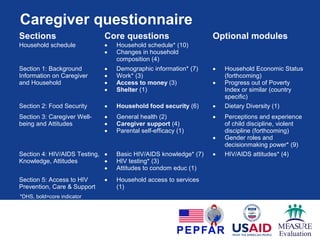
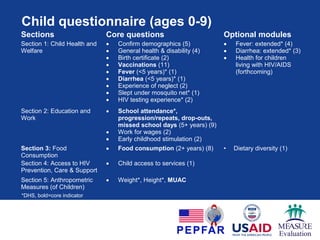
The document evaluates the impact of Orphan and Vulnerable Children (OVC) programs by proposing standardized survey tools aimed at improving child and caregiver well-being data collection. It identifies a gap in existing measurement tools and outlines a structured process for developing core indicators and questionnaires for various stakeholders involved in OVC programming. The tools are designed for population-level assessments to enable informed programming and mid-course corrections, with a focus on identifying the outcomes of interventions across diverse regions and demographics.