3
Outline
Objective
Introduction
Definition of inductionand augmentation of labor
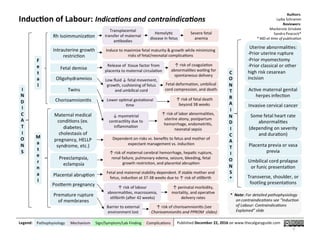
Indications and contraindications for labor induction
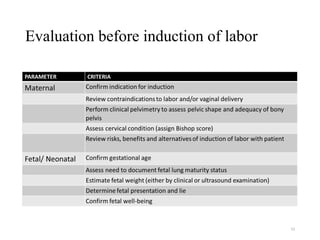
Evaluation before Induction of Labor
Methods of cervical ripening and induction of labor
Complications of induction and augmentation
References
4.
4
Objectives
At the endof this presentation you will be able to:
•Define the term induction and augmentation
•Know Indication and contraindication of induction
•Understand way of predicting successful induction
•Know pharmacological and mechanical way of cervical
ripening and induction of labor
•Know both maternal and fetal complications after inducing
or augmenting labor
5.
5
DEFINITION
Induction of labor
•Artificialinitiation of uterine contractions before the
onset of spontaneous labor to accomplish vaginal
delivery.
Augmentation of labor
•Increasing the frequency and improving the intensity
of existing uterine contractions in a patient who is in
labor and not progressing adequately, in order to
accomplish vaginal delivery.
6.
6
Introduction
One ofthe most frequently done procedures to
manage labor & delivery.
Done when the benefits of delivery to the fetus or
the mother exceed the benefits of continuing the
pregnancy.
7.
7
Undertaken when bothof the following criteria
are met :
1. If continuation of the pregnancy is associated with
greater maternal/fetal risk than the risk of
intervention to deliver the pregnancy
2. There is no contraindication to Vaginal birth
8.
8
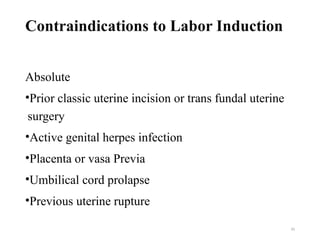
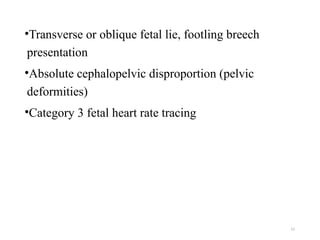
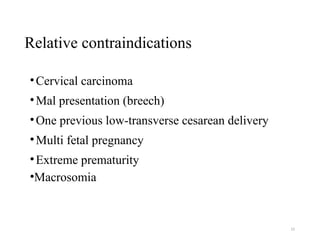
Indications and contraindicationsfor
labor induction
Factors determining indications can be categorized
into :
maternal and fetal conditions
gestational age
cervical status
other factors
14
Elective induction oflabor
•Elective induction of labor refers to the initiation of
labor for convenience in an individual with a term
pregnancy who is free of medical or obstetric
indications
15.
15
•Although elective inductionat or after 39 weeks of
gestation is not recommended, it may be appropriate in:
women with a history of very short labors
who live a great distance from the hospital
who has experienced a prior stillbirth at or near term
to ease anxiety and fears about the loss of a
subsequent pregnancy
when a fetal anomaly is present.
16.
16
Prediction of laborinduction success
characteristics associated with successful induction
include:
•Multiparty
•Tall stature (over 5 feet 5inches)
•Increasing gestational age
•Non obese maternal weight or body mass index
•Infant birth weight less than 3.5 kg
•Elevated fetal fibronectin (fFN) concentration in
cervicovaginal secretions
•Sonographically measured short cervical length
17.
17
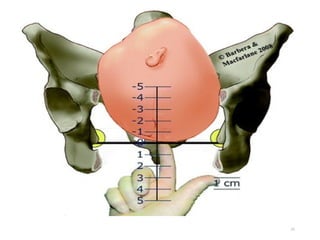
•Cervical status isone of the most important factors for
predicting successful induction of labor
•The modified Bishop score syste is most commonly
used in clinical practice to evaluate the cervix prior to
induction.
- It tabulates a score based upon the station of the
presenting part and four characteristics of the cervix:
dilatation, effacement, consistency, and position
22
Requirements For CervicalRipening And
Induction Of Labor
a) Personnel familiar with the effects of uterine
stimulants on the mother and fetus because uterine
hyper stimulation may occur with induction of labor.
b) Monitoring fetal heart rate and uterine contractions
is recommended as for any high-risk patient in
active labor.
c) A physician capable of performing a cesarean
delivery should be readily available.
23.
23
Labor induction isprimarily conducted by using
amniotomy, prostaglandins, and oxytocin, each alone
or in combination
Methods of cervical induction
24.
24
1. Prostaglandins
• PGsare endogenous compounds found in the
myometrium, deciduas, and fetal membranes during
pregnancy
• Side effects: chills, fever, vomiting, diarrhea
• Contraindications: renal and liver dysfunctions, asthma
25.
25
PGE2 (Dinoprostone)
a. 0.5mg in 2.5 ml gel (prepidil)
Intracervical
Q 6 – 12 hrs
Max. 1.5 mg/24 hrs till Cx ripening
Induction 6 – 12 hrs after last dose
b. 10 mg vaginal insert (Cervidil)
Timed release (0.3 mg/hr)
Leave in place for 12 hrs
Induction with oxytocin 30 – 60’ after
removal
26.
26
Prostaglandin E1
Misoprostol (cytotec)
Bothvaginal and oral misoprostol are used for
either cervical ripening or labor induction.
Synthetic prostaglandin E1 analog available as
100 mcg and 200 mcg tablets
25 mcg, intra-vaginal into posterior fornix
Q 3 – 6 hrs till the Cervix becomes favorable
Induction 4 hrs after the last dose
27.
27
2.Synthetic oxytocin
Oxytocin isa polypeptide hormone produced in the
hypothalamus and secreted from the posterior lobe of the
pituitary gland in a pulsatile fashion
Synthetic oxytocin an effective means of labor induction
Effect first demonstrable from 20 wks onwards
Given intravenously/intramuscularly
The plasma half life estimated at 3 to 6 minutes
Steady-state concentrations reached within 30 to 40 minutes
of initiation
Dilution: 10 IU in 1000ml of isotonic IV fluid; 10mu/ml &
given by infusion pump or drip form
28.
28
3. Amniotomy
Elective amniotomywith the intention of accelerating
labor is often performed.
Amniotomy at approximately 5-cm dilation accelerated
spontaneous labor by 1 to 1½ hours.
Amniotomy is associated with a risk of cord prolapse.
To minimize this risk, disengagement of the fetal head
during amniotomy is avoided and
Fundal or suprapubic pressure or both may be helpful.
29.
29
Care during inductionof labor
Informed consent by the woman
reasons for induction
choice of method to be used
potential risks and consequences of accepting or declining
an offer of induction of labor.
Oxytocin infusion is discontinued whenever hyperstimulation
or fetal distress is identified but can be restarted when
reassuring fetal heart rate and uterine activity patterns are
restored.
30.
30
Cont.
Place of induction
shouldoccur on a delivery suite
continuous electronic monitoring of both FHR and uterine
activity
Women receiving oxytocin for induction of labor should
receive one-to-one follow up care.
Following instillation of prostaglandin agents, the woman
should be advised to lie down for at least 30 minutes
31.
31
Cont.
Fetal surveillance
continuous uterineand FHR monitoring
Fetal wellbeing should be established immediately prior to
induction of labor.
FHR and uterine activity should be monitored continuously
for a period of 30 minutes to 2 hours after administration of
the PGE2
FHR monitoring continued if regular uterine contractions
persist;
Where oxytocin is being used for induction labor,
continuous electronic fetal monitoring should be used.
33
Uterine over activity
•Uterine tachysystole is defined as 6 contractions in a 10-
minutes in consecutive 10-minute intervals
• Uterine hypertonus is described as a single contraction lasting
longer than 2 minutes in a 10-minute period
• Uterine hyperstimulation is when either condition leads to a
nonreassuring fetal heart rate pattern
• Non reassuring : demonstrated by late deceleration, or fetal
bradycardia
Concurrent administration of oxytocin and a prostaglandin
increase the risk of tachysystole
34.
34
Failed induction
• Thereare various ways to define failed induction but it is
important to allow adequate time for cervical ripening and
development of an active labor pattern before determining
that an induction has failed.
• The inability to achieve cervical dilatation of 4 cm and 80%
effacement or 5 cm (regardless of effacement) after a
minimum of 12 to 18 hours of both oxytocin administration
and membrane rupture.
• Uterine contractions should reach 5 in 10 minutes or 250
Montevideo units, which is the minimum level achieved by
most women whose labor is progressing normally.
















![Abnormal Labor [ Natnael Dechasa Gemeda pdf ].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/abnormallabornatnaeldechasagemedapdf-230317103358-a4021124-thumbnail.jpg?width=640&height=640&fit=bounds)













![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















