Download to read offline


















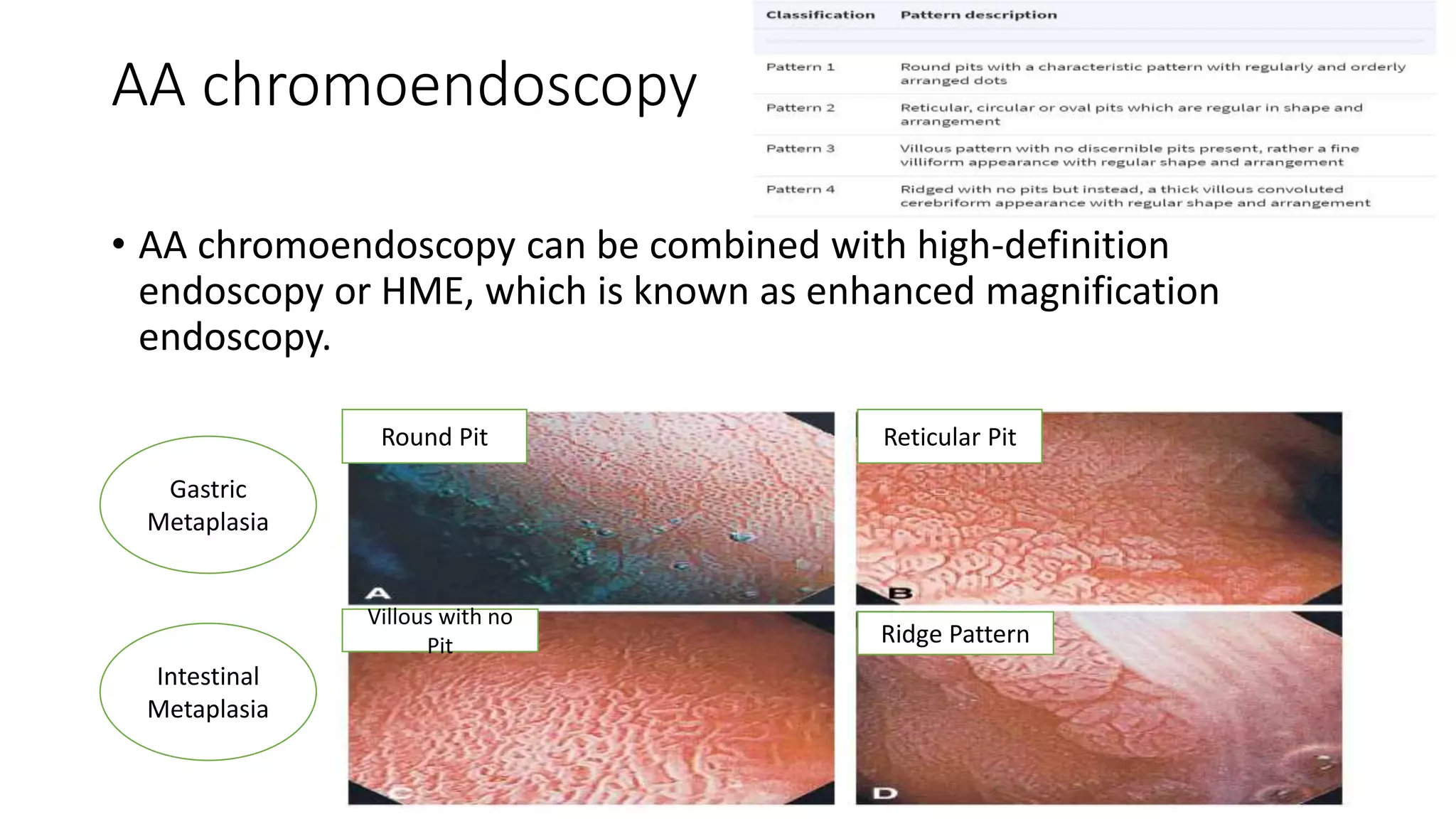




































This document discusses oesophageal endoscopy procedures and their uses. It covers the anatomy and technology behind endoscopes, as well as various diagnostic and therapeutic applications. Key points include: - Endoscopy has advanced from a purely diagnostic tool to one capable of various therapies for conditions like GERD, achalasia, and obesity. - Imaging technologies like chromoendoscopy and narrow band imaging help detect early neoplastic lesions and distinguish between dysplastic and non-dysplastic tissue. - Endoscopy is used to diagnose and treat conditions that cause dysphagia like peptic strictures, Schatzki rings, eosinophilic esophagitis, and post-surgical an


































![OESOPHAGEAL ANATOMY AND PATHOLOGIES (2) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/oesophagealanatomyandpathologies2autosaved-250917094352-40c57836-thumbnail.jpg?width=640&height=640&fit=bounds)








































