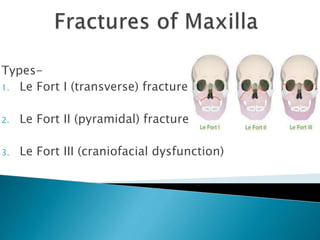
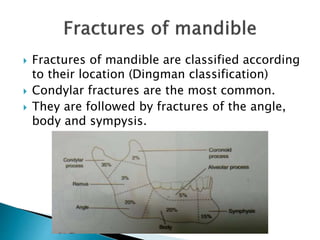
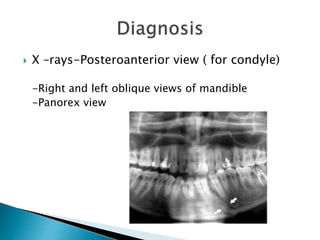
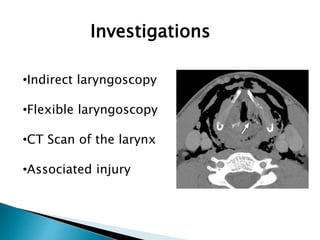
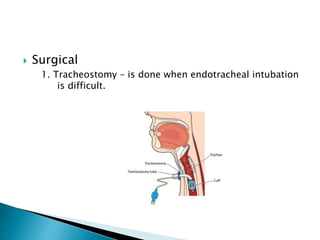
This document summarizes common ENT injuries seen in polytrauma patients. It discusses nasal bone fractures, maxillary fractures, mandible fractures, and temporal bone fractures. For each type of injury, it outlines clinical presentations, investigations, classification, and treatment approaches including closed or open reduction techniques. It also reviews laryngotracheal trauma including associated clinical features, investigations, and management strategies such as conservative treatment with steroids or surgical interventions like tracheostomy or open reduction with internal fixation.





















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















