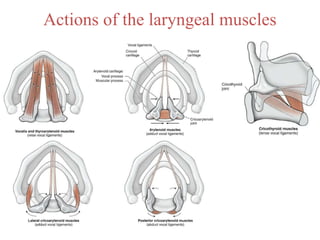
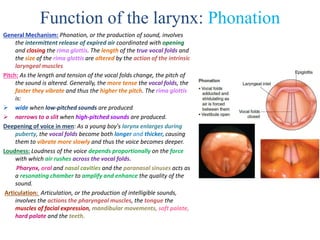
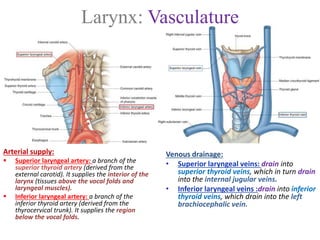
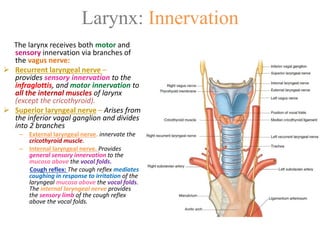
The larynx is a complex structure comprising multiple cartilages that plays a crucial role in breathing, phonation, and protecting the airway. It consists of unpaired cartilages (thyroid, cricoid, epiglottis) and paired cartilages (arytenoid, corniculate, cuneiform), with various ligaments and muscles supporting its functions. The larynx is richly innervated and vascularized, and has significant clinical implications, particularly in emergencies requiring procedures like cricothyrotomy.