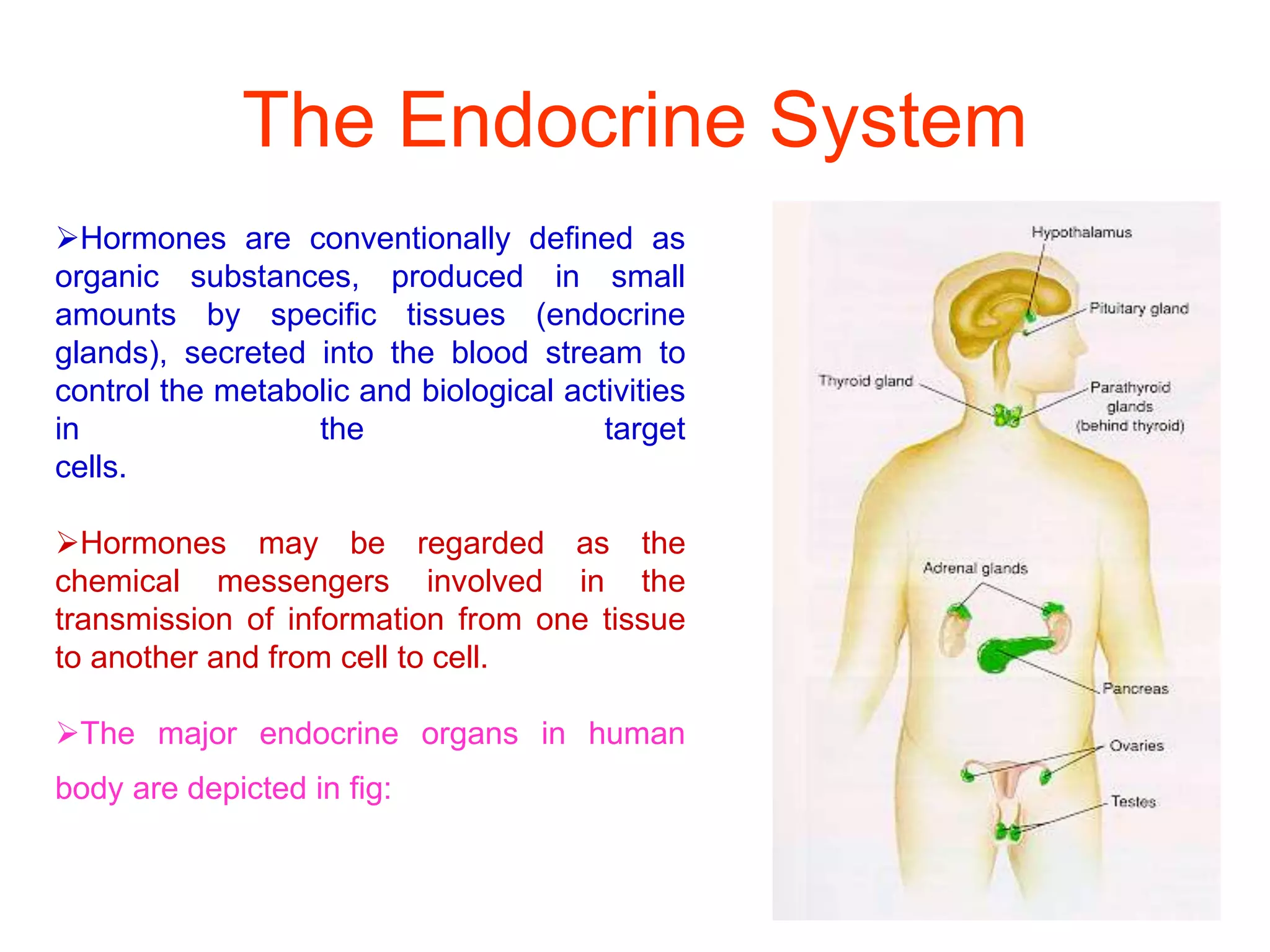
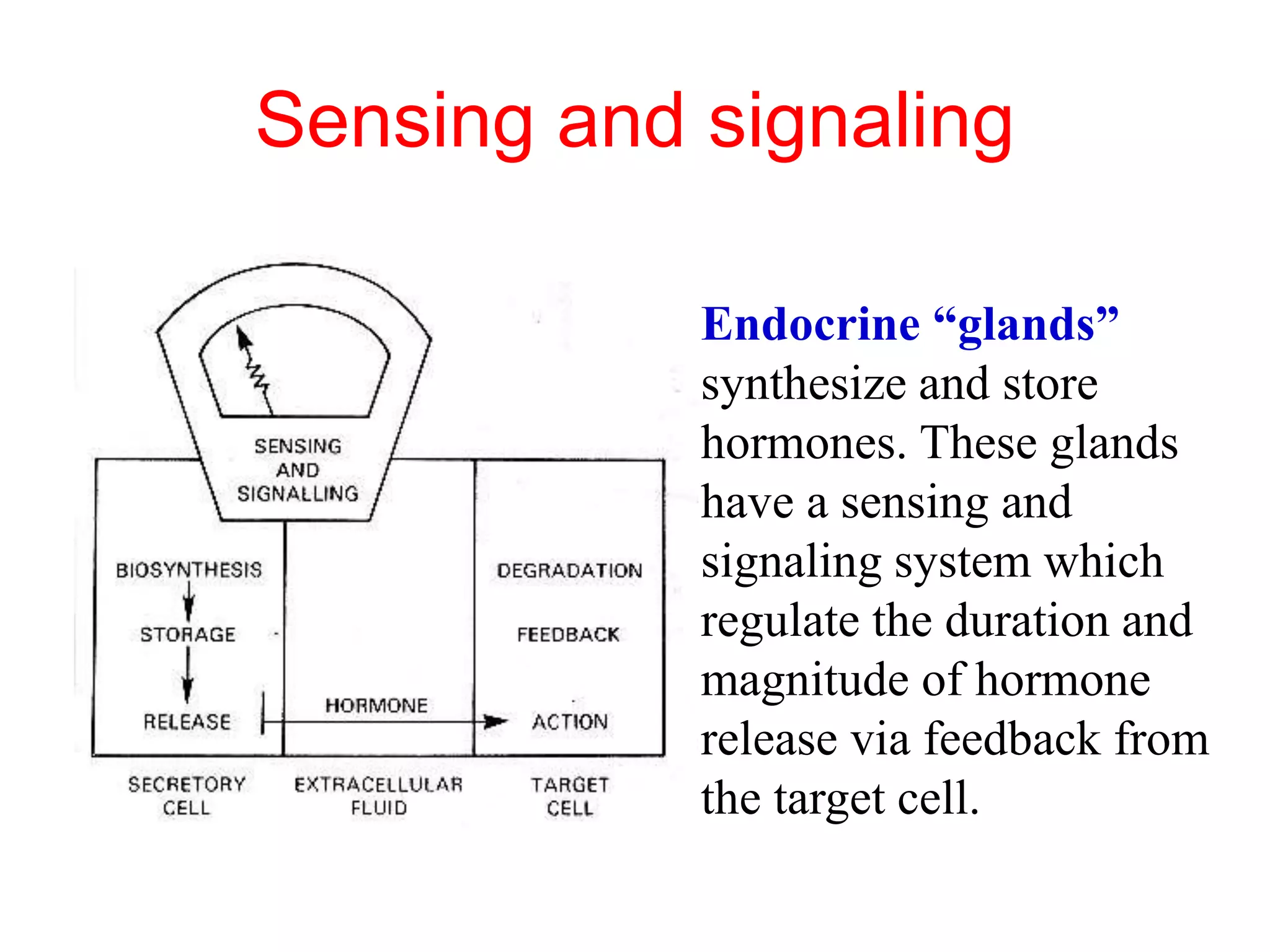
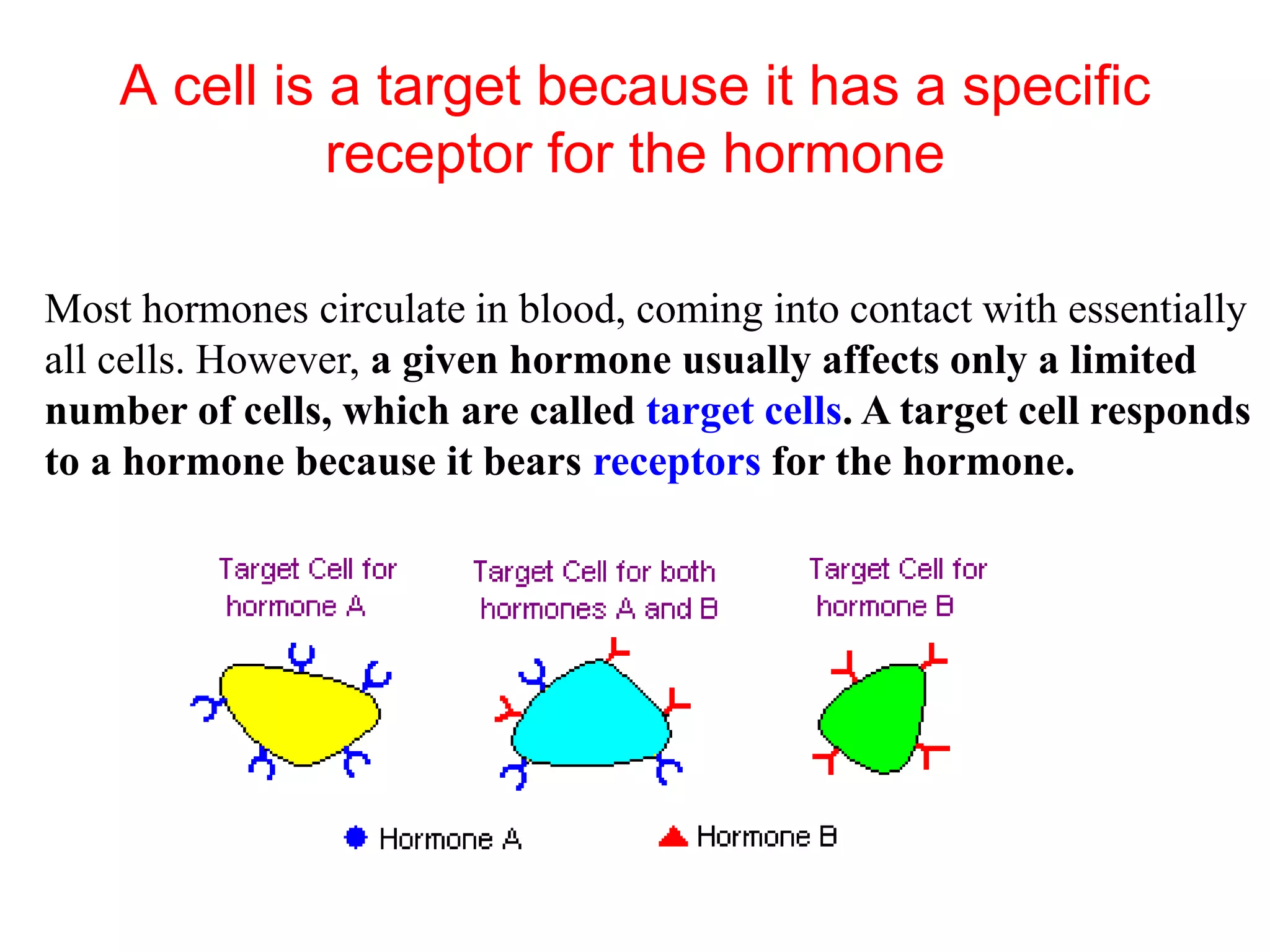
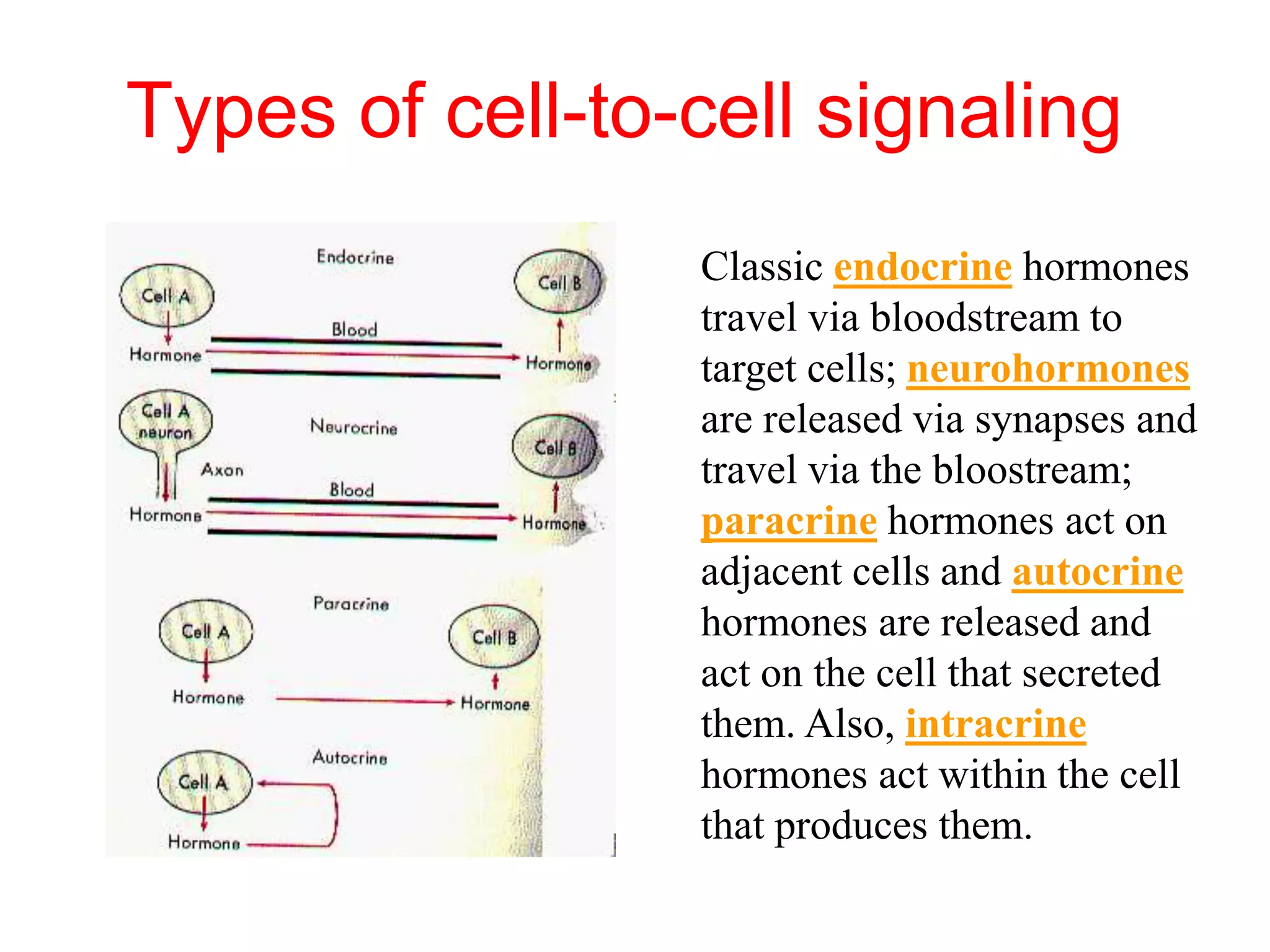
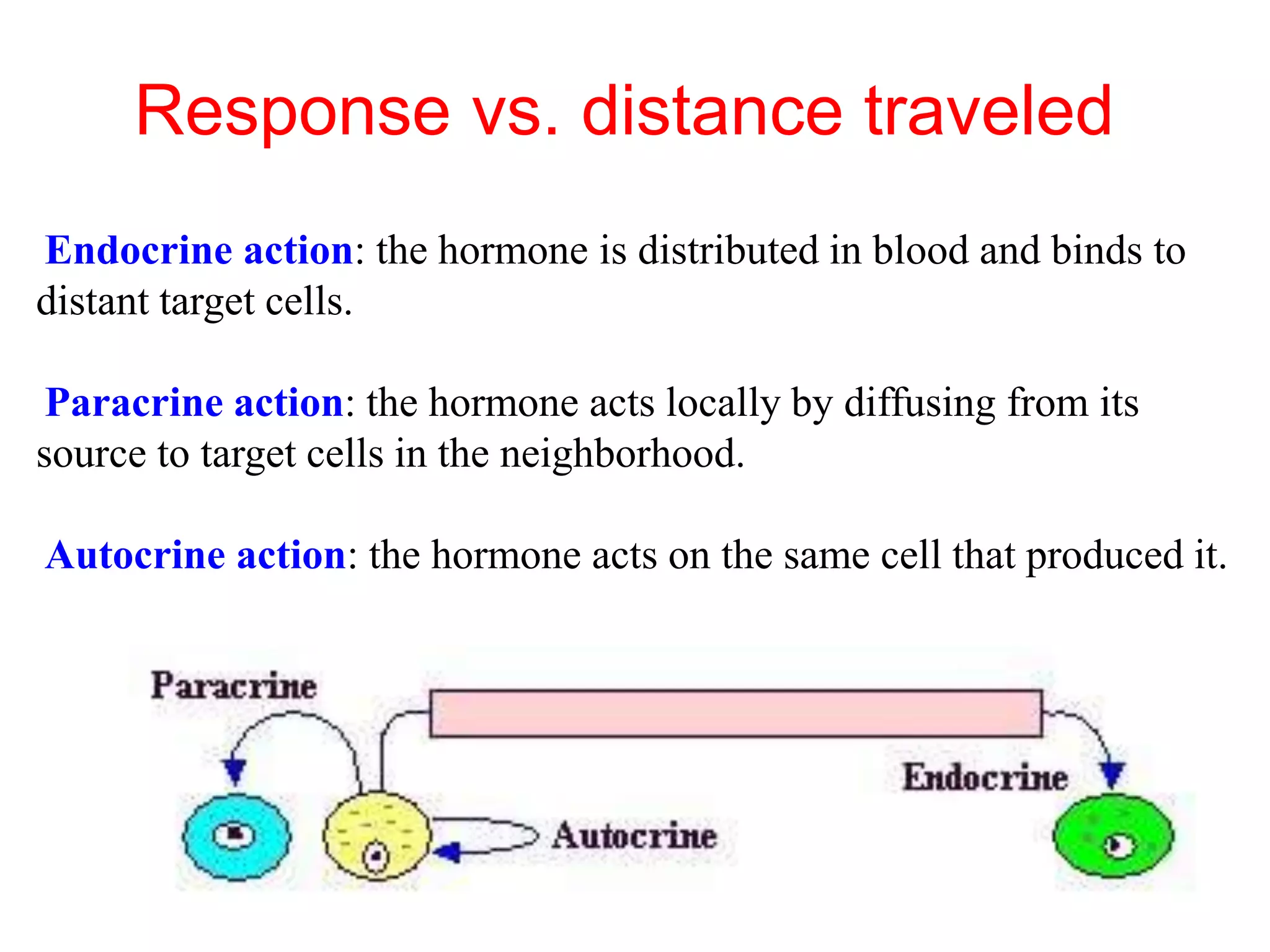
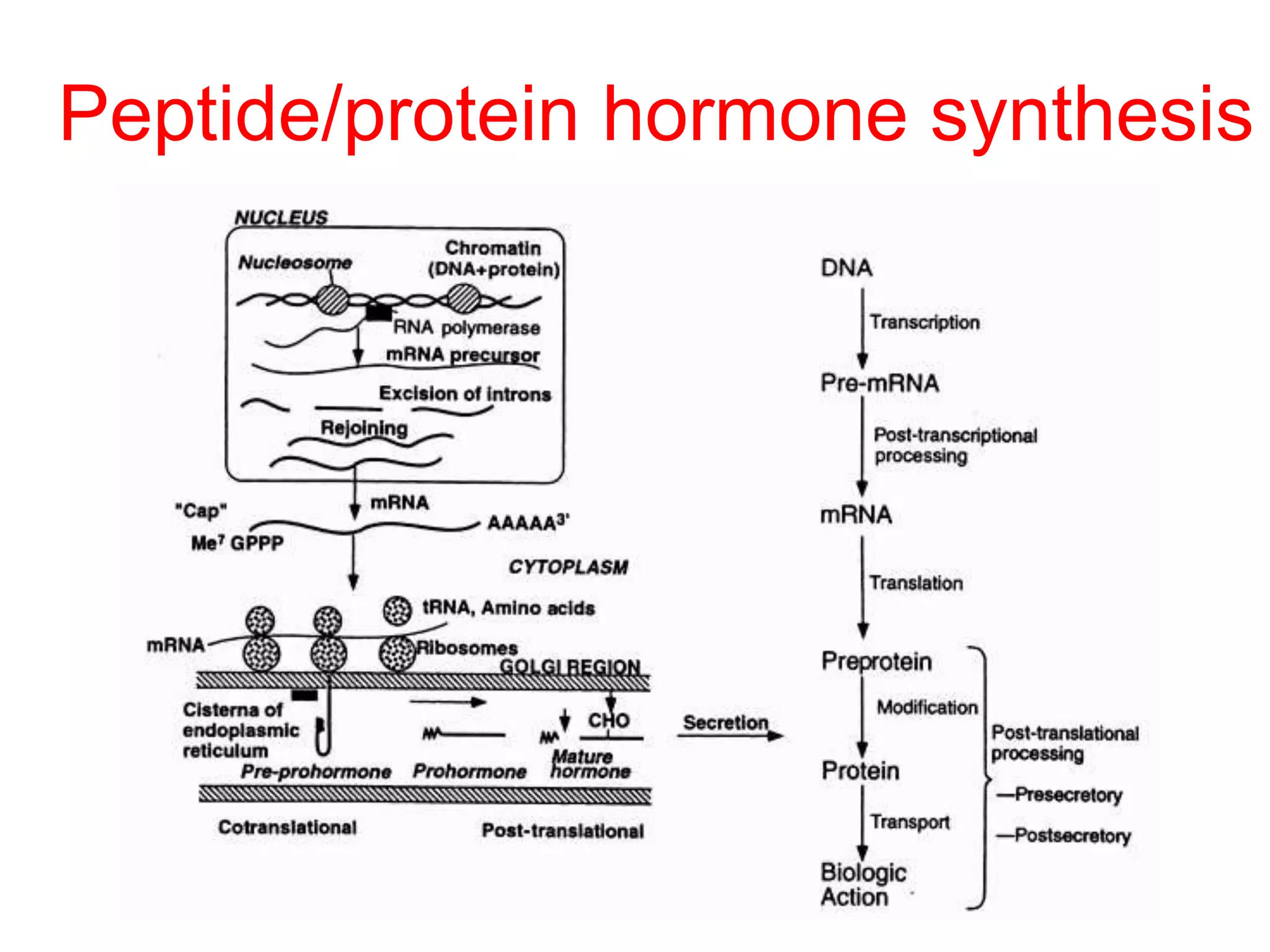
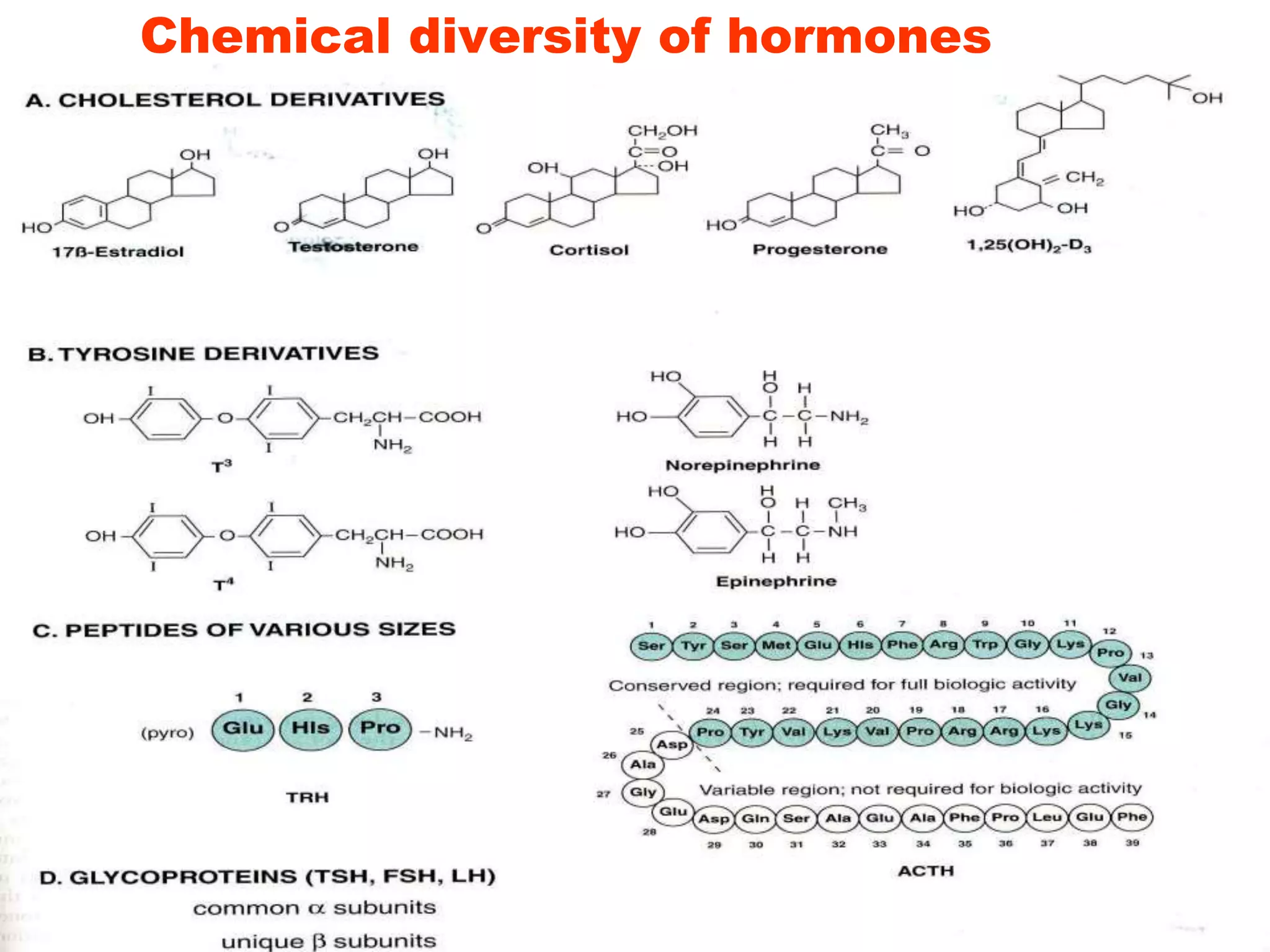
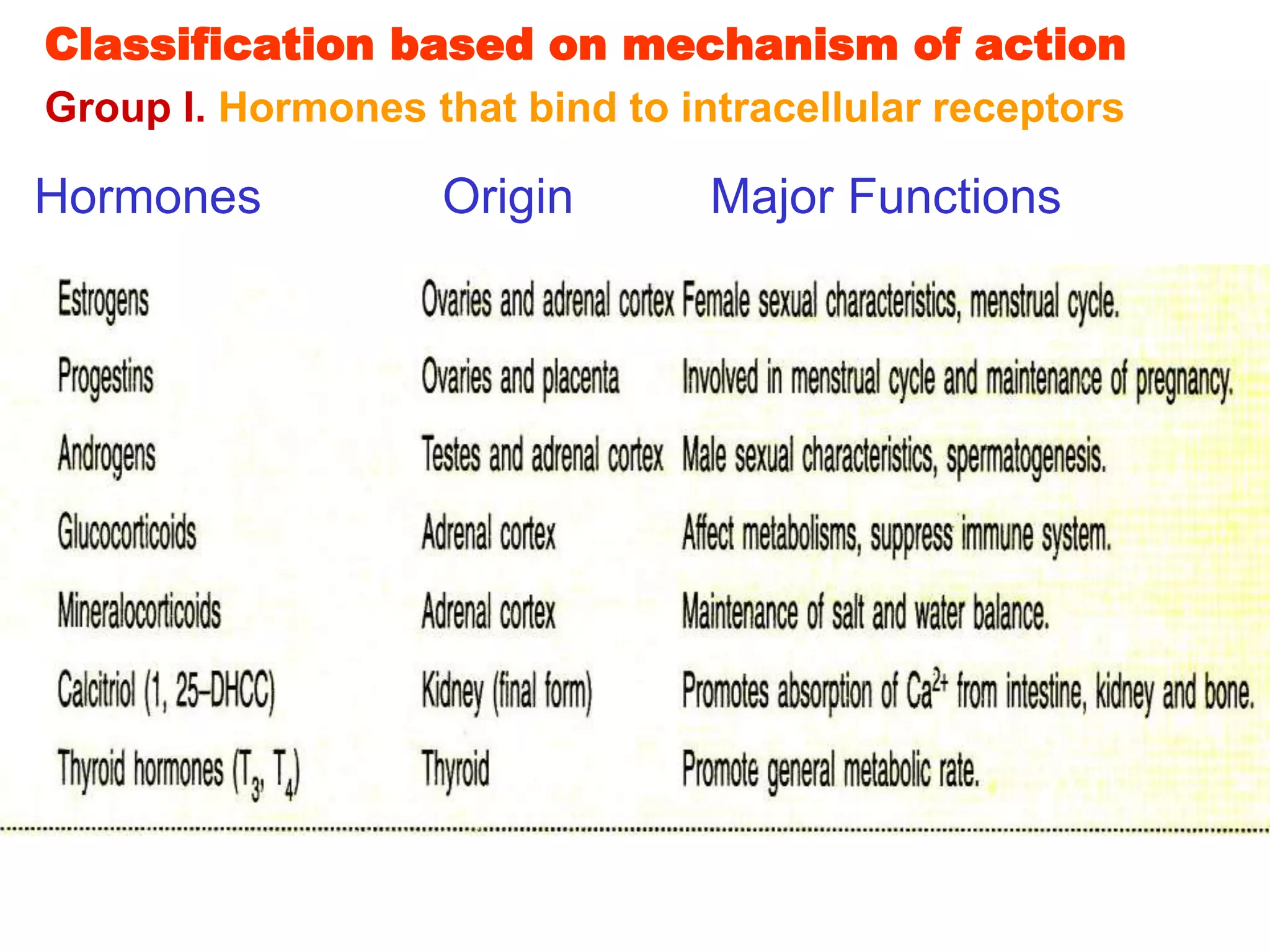
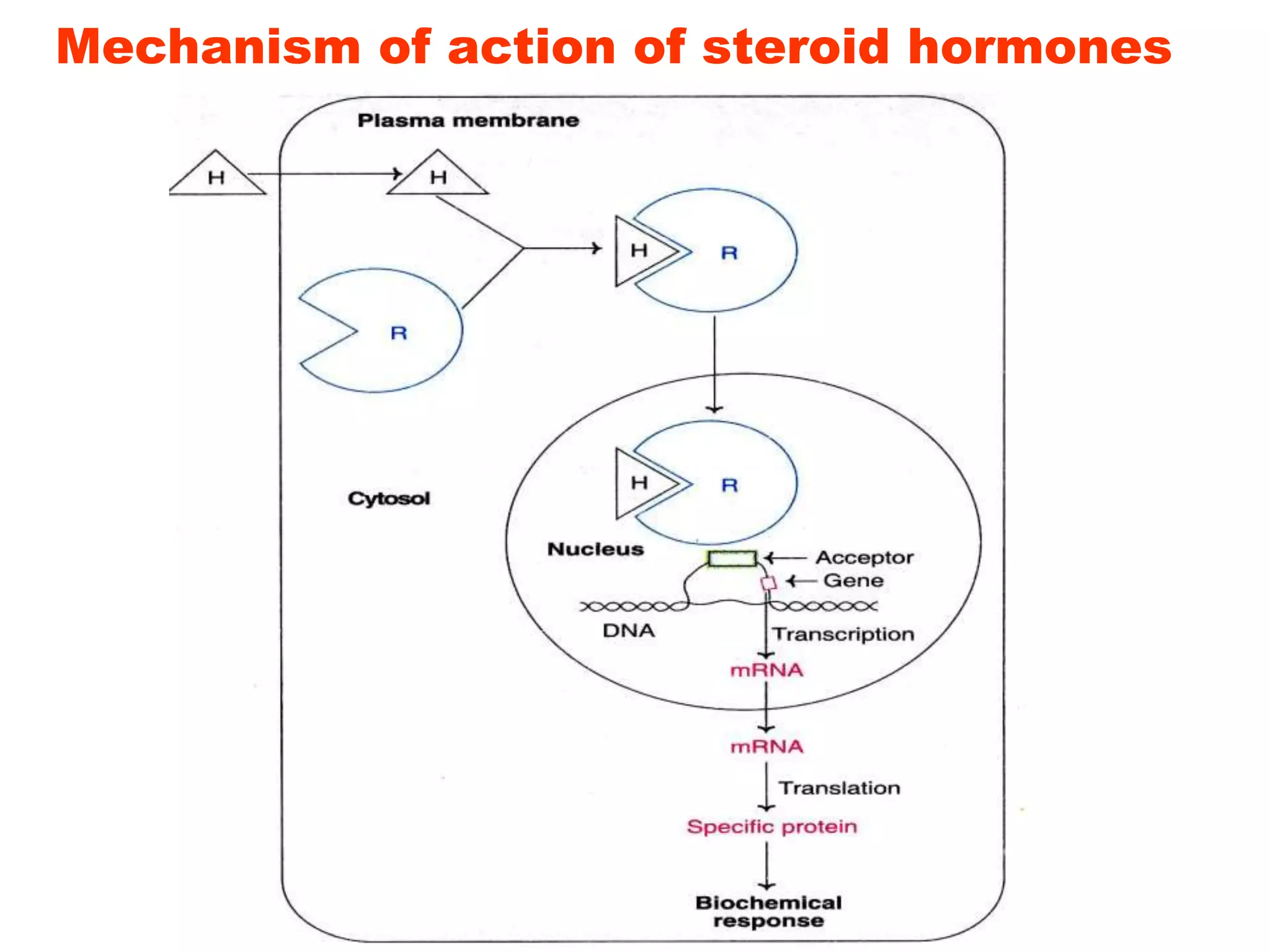
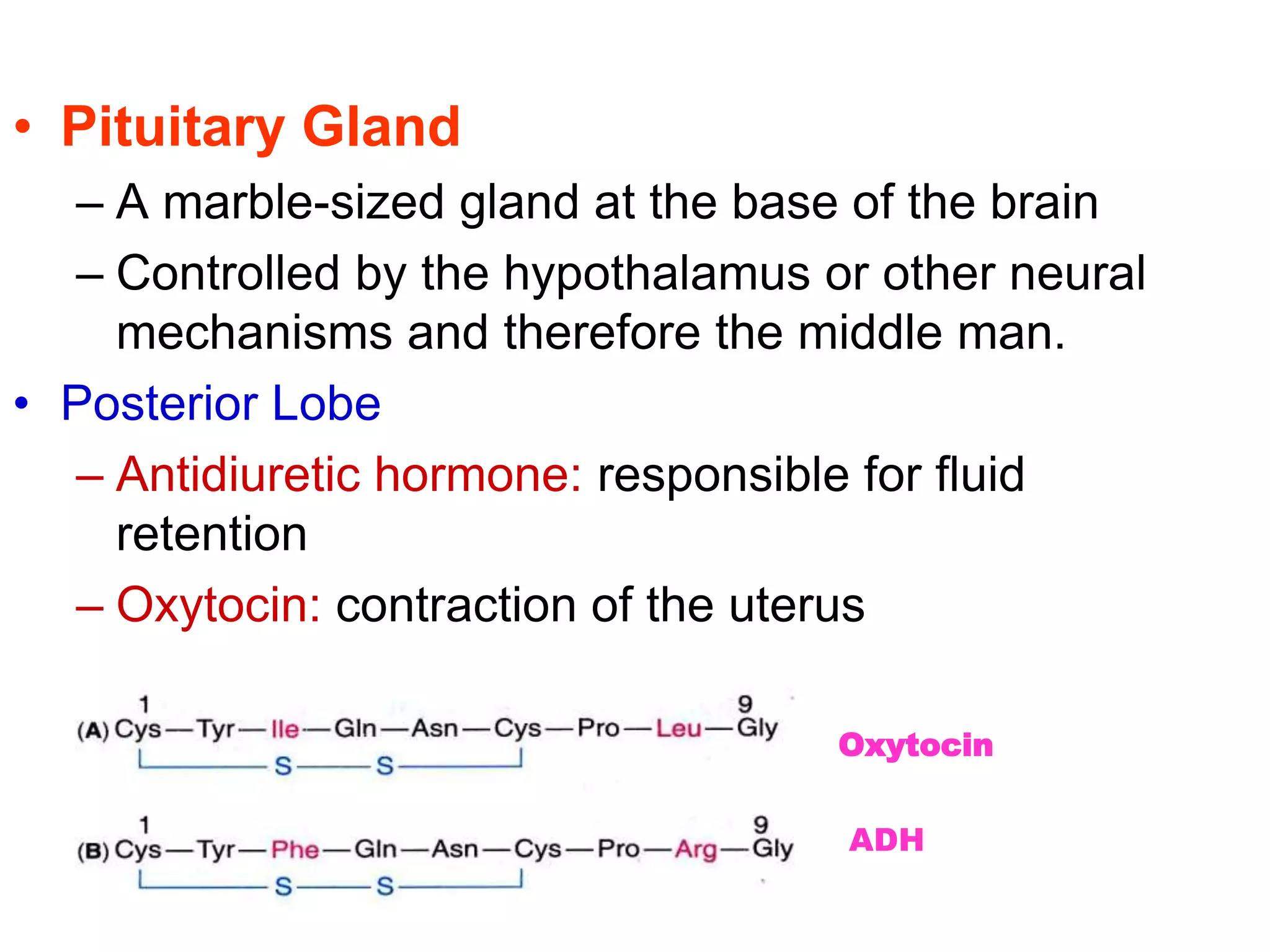
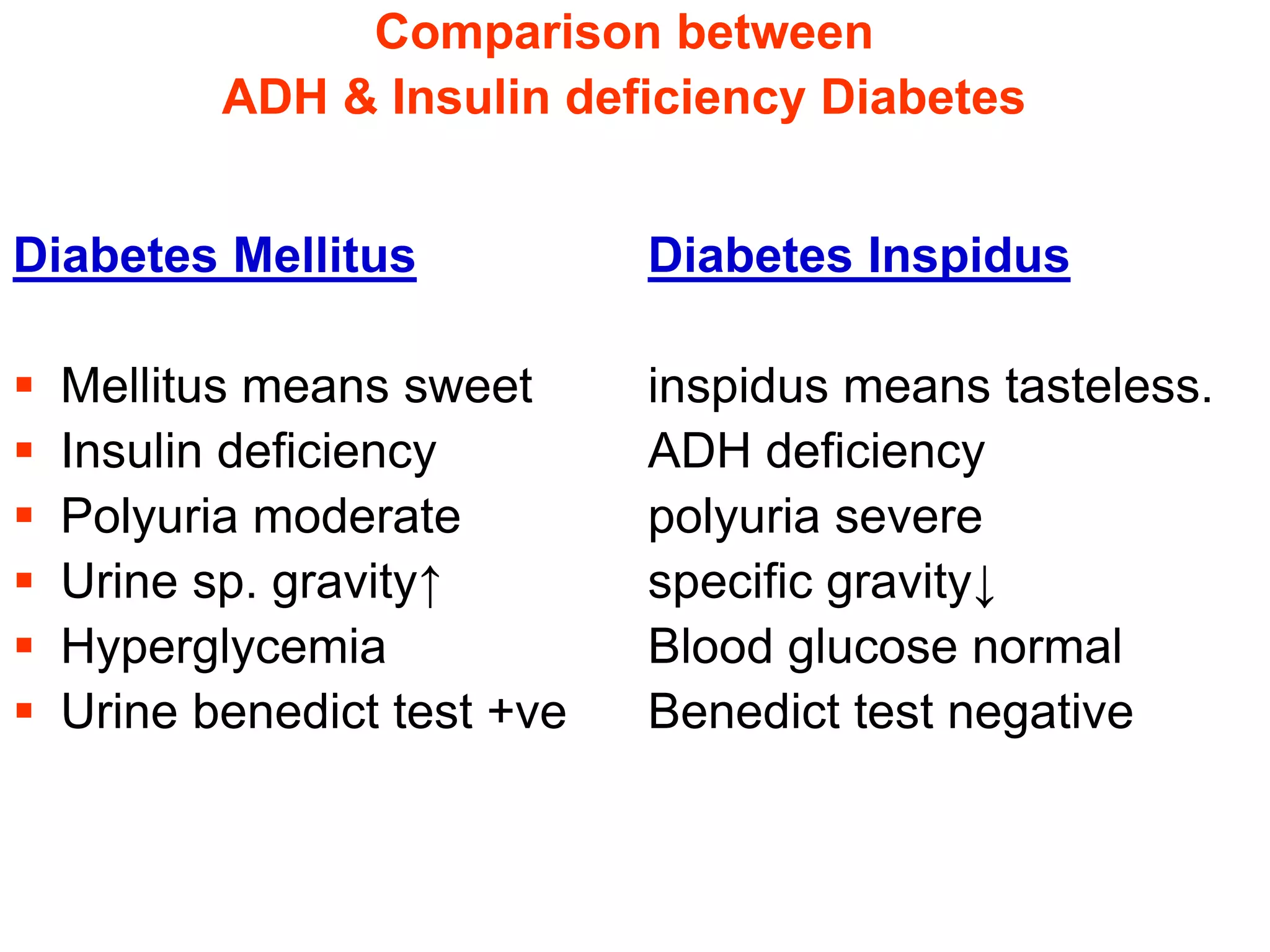
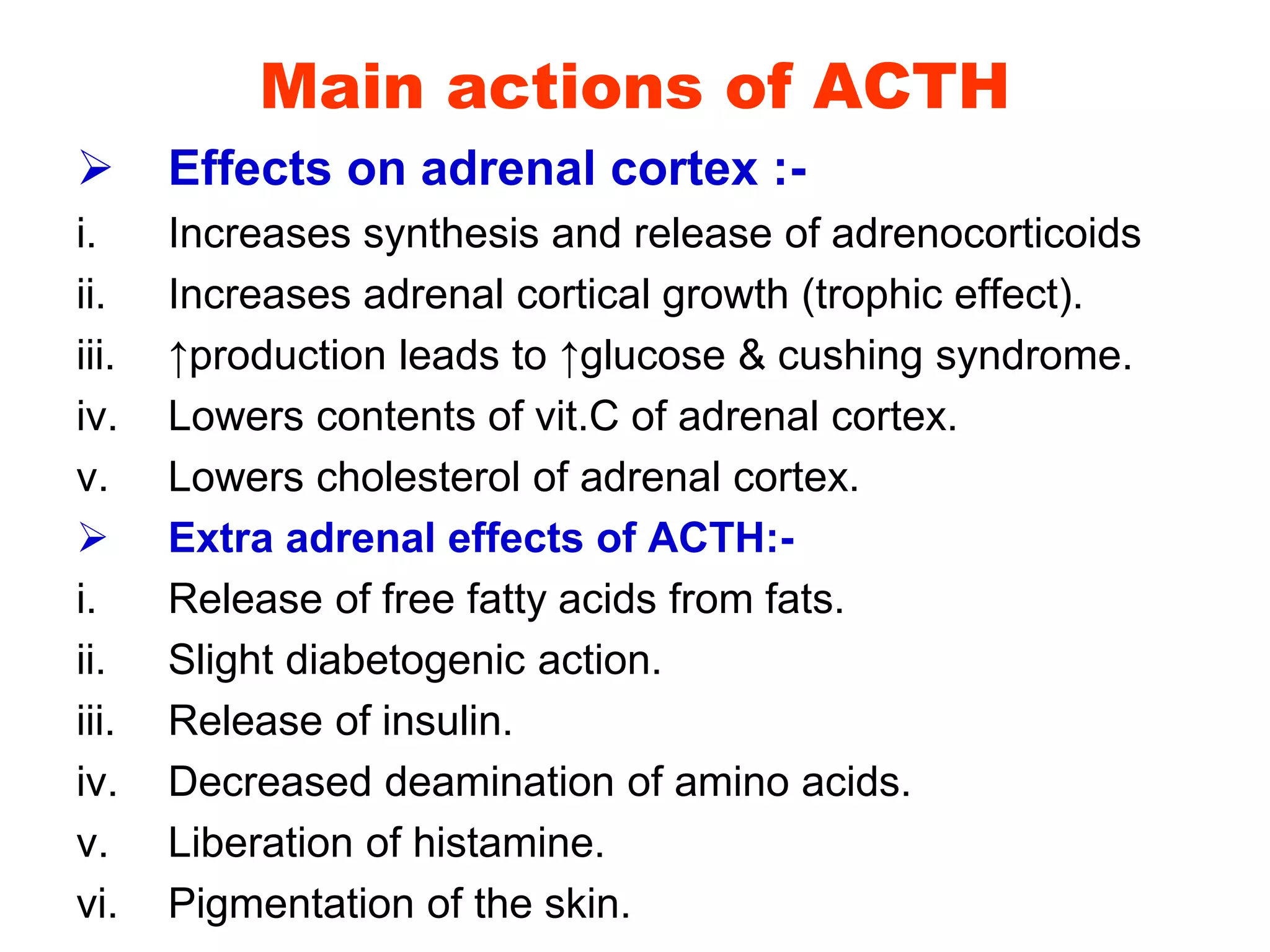
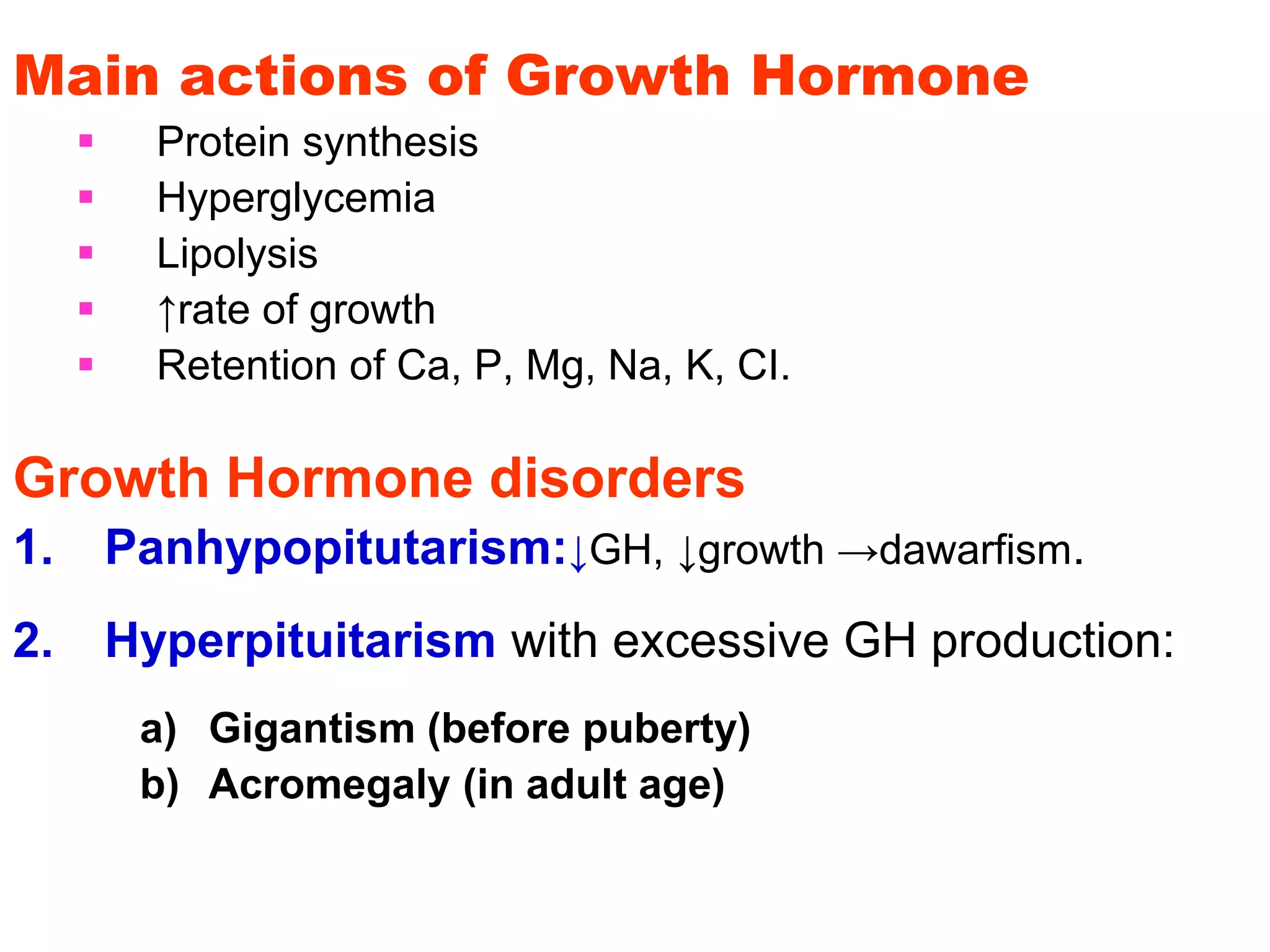
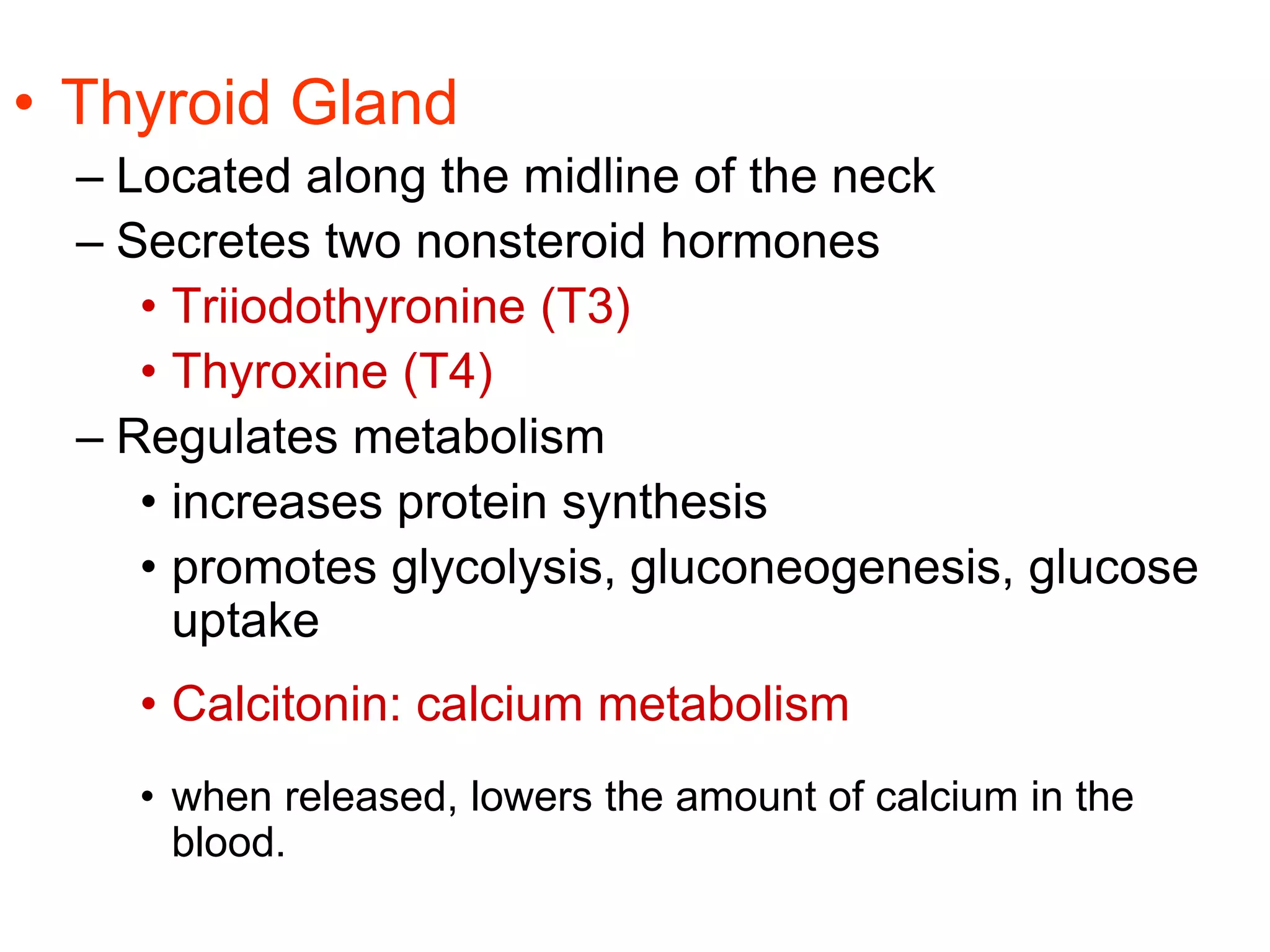
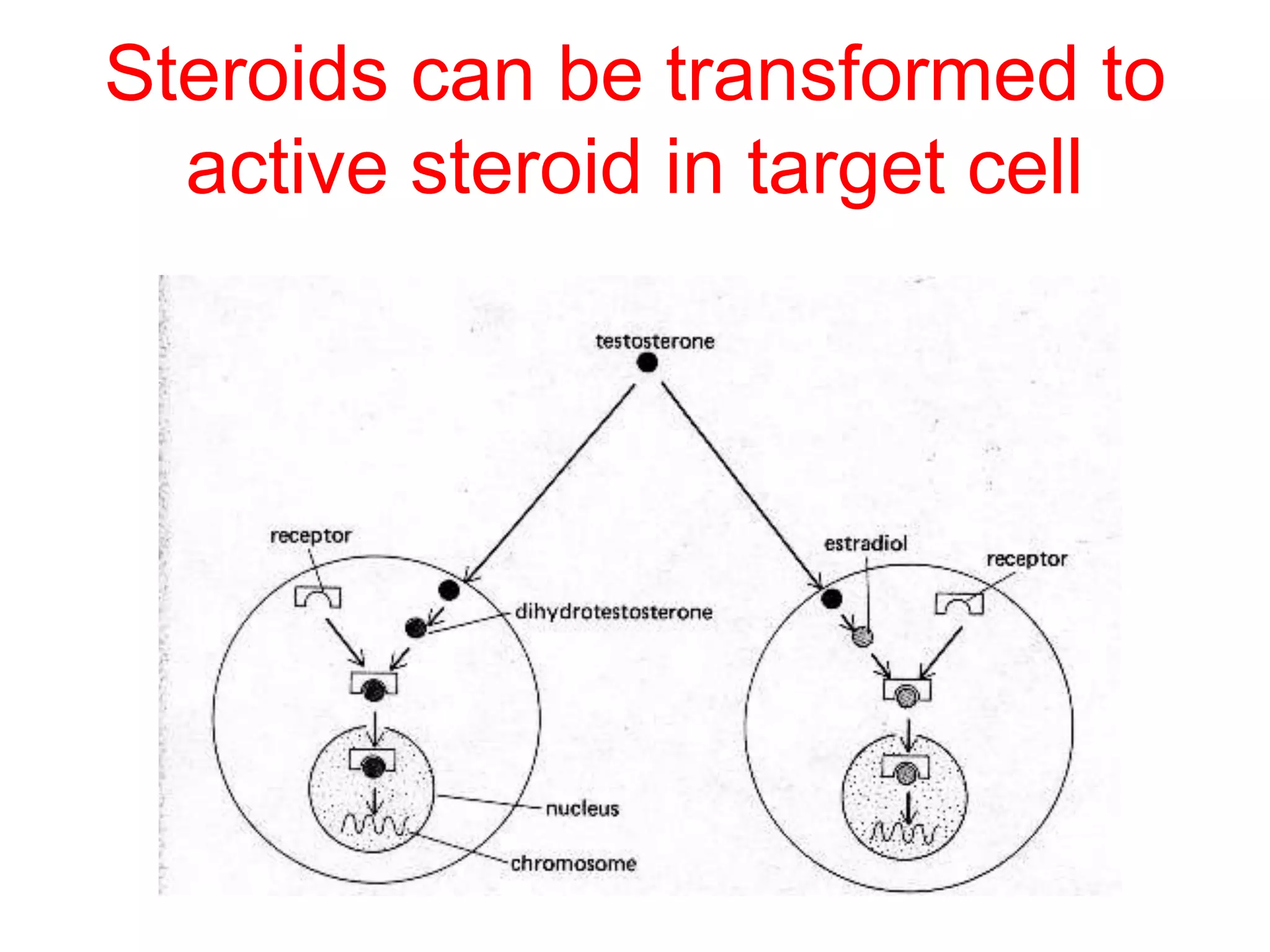
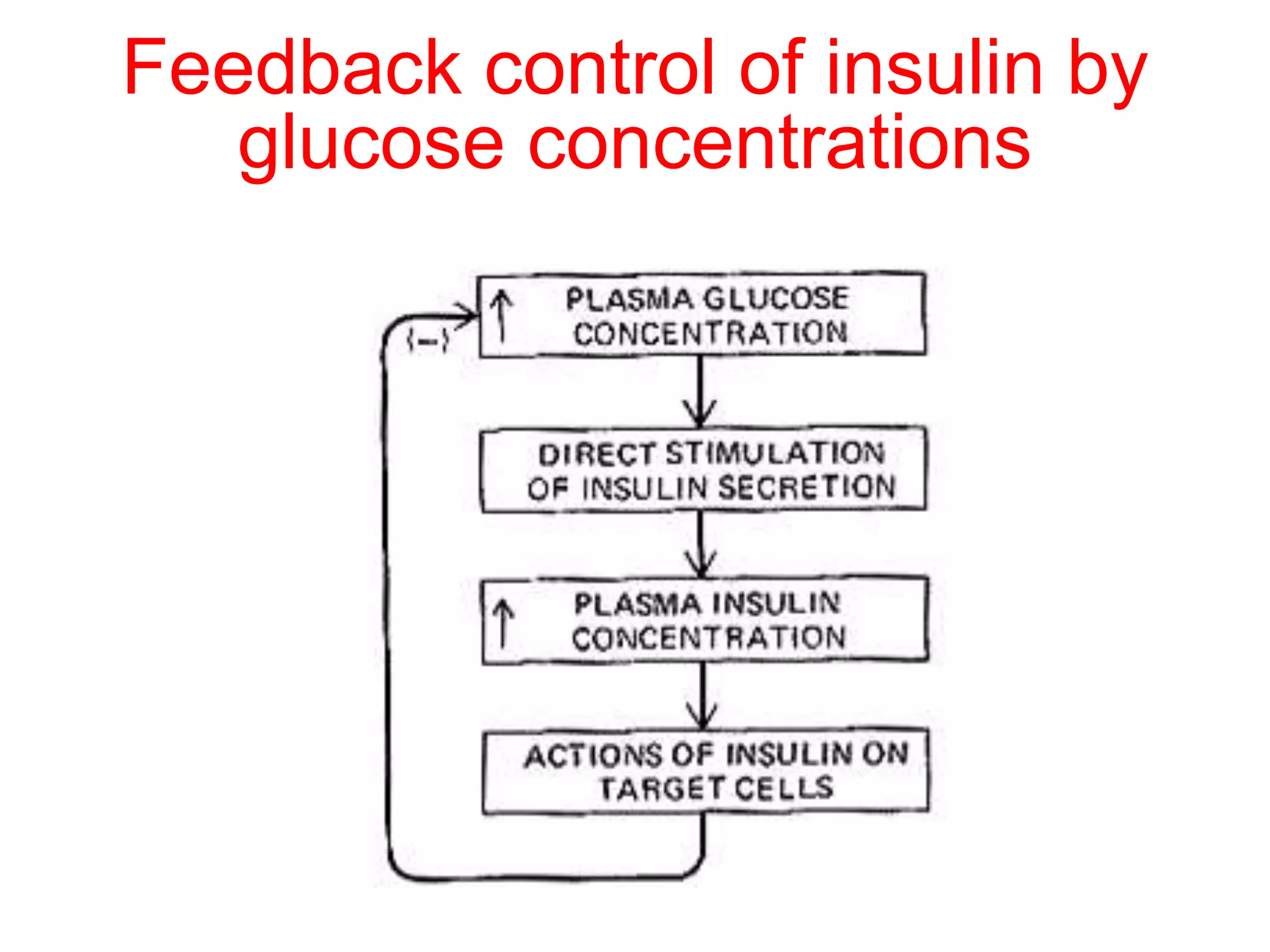
The document discusses the endocrine system, which regulates homeostasis through the secretion of hormones directly into the bloodstream. It describes the major endocrine glands and hormones, including the hypothalamus and pituitary gland which regulate other glands. The hormones act on target cells through various mechanisms, such as binding to intracellular receptors to activate genes or binding to cell surface receptors and triggering secondary messengers like cAMP. The endocrine system works in tandem with the nervous system to coordinate bodily functions.