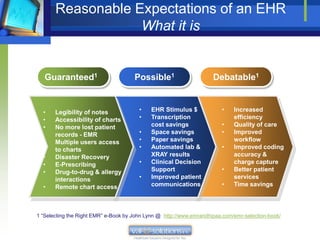
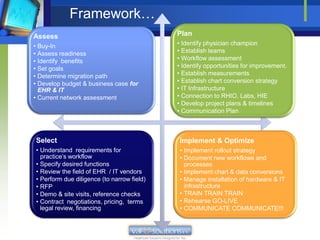
The document outlines the transition from paper-based systems to electronic health records (EHR), detailing the phases involved and the benefits of EHR implementation. It discusses common misconceptions, critical success factors, and meaningful use criteria necessary for healthcare providers to optimize their use of EHR systems. Additionally, it provides a checklist and encourages collaboration among various stakeholders to achieve successful EHR implementation and adoption.












































![13 core objectives to achieve meaningful use stage1 [Infographic]](https://cdn.slidesharecdn.com/ss_thumbnails/13coreobjectivestoachivemeaningfulusestage1-150226075252-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)






























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














