Downloaded 23 times

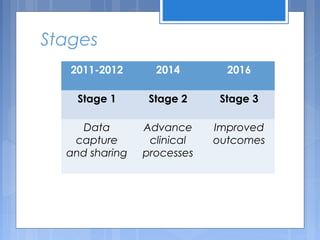
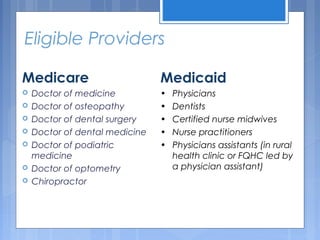
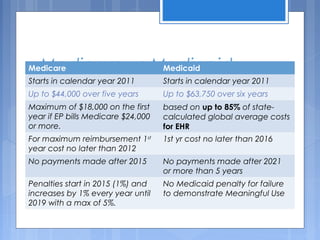



The document discusses the concept of 'meaningful use' in healthcare, which involves using certified electronic health record (EHR) technology to enhance quality, safety, and efficiency while engaging patients and maintaining privacy. It outlines various objectives and stages of meaningful use, detailing incentives for eligible providers under Medicare and Medicaid, along with compliance requirements and potential audits. Key information about attestation, penalties, and applicable laws is also included, emphasizing the importance of documentation and adherence to regulations.



































![13 core objectives to achieve meaningful use stage1 [Infographic]](https://cdn.slidesharecdn.com/ss_thumbnails/13coreobjectivestoachivemeaningfulusestage1-150226075252-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)


















![Cms+ehr incentive program_hospital_training_final[1]](https://cdn.slidesharecdn.com/ss_thumbnails/cmsehrincentiveprogramhospitaltrainingfinal1-101130114653-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



















































