Downloaded 44 times

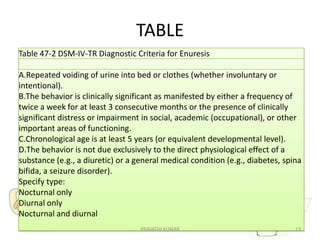


This document discusses two elimination disorders: encopresis and enuresis. Encopresis is defined as involuntary fecal soiling. It is usually caused by constipation and overflow incontinence beginning in early childhood. Treatment involves addressing constipation medically as well as behavioral interventions. Enuresis is defined as involuntary urination, especially at night. It is developmentally normal in young children but considered a disorder after age 5. Genetic factors and developmental delays may contribute to enuresis. Diagnosis involves recurrent urinary accidents at least twice a week for over 3 months in a child over age 5.








































































![Chapter 39 role of radiotherapy in benign diseases.pptx [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter39roleofradiotherapyinbenigndiseases-191105205437-thumbnail.jpg?width=640&height=640&fit=bounds)































