GENERAL
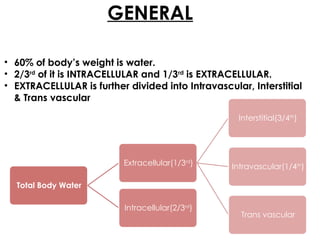
• 60% ofbody’s weight is water.
• 2/3rd
of it is INTRACELLULAR and 1/3rd
is EXTRACELLULAR.
• EXTRACELLULAR is further divided into Intravascular, Interstitial
& Trans vascular
Total Body Water
Extracellular(1/3rd
)
Interstitial(3/4th
)
Intravascular(1/4th
)
Trans vascular
Intracellular(2/3rd
)
4.
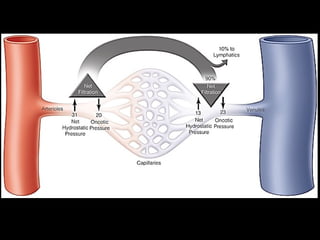
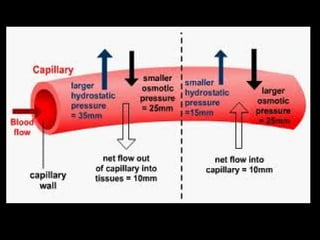
NORMAL FLUID CIRCULATION
The movement of fluid between vasculature is
controlled by opposing effects of “Vascular
Hydrostatic Pressure” & “Plasma Colloid Osmotic
Pressure”.
Hydrostatic Pressure is more at the Arteriolar end
whereas Oncotic pressure is more at the Venous end.
Exit of fluid from arteriolar end is balanced by inflow at
venular end of microcirculation.
Small residual amount of excess interstitial fluid is
drained by lymphatics.
6.
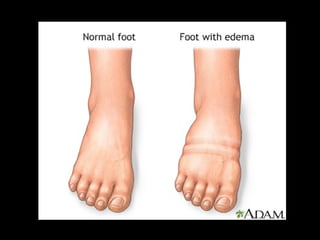
EDEMA
Edema isan abnormal accumulation of fluid in the
interstitium, located beneath the skin and in the
cavities of the body.
Edema is a normal response of the body to
inflammation or injury. For example, a twisted ankle, a
bee sting, or a skin infection will all result in edema in
the involved area.
In some cases, such as in an infection, this may be
beneficial. Increased fluid from the blood vessels
allows more infection-fighting white blood cells to
enter the affected area.
8.
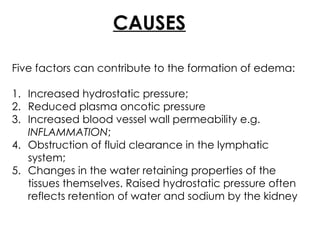
CAUSES
Five factors cancontribute to the formation of edema:
1. Increased hydrostatic pressure;
2. Reduced plasma oncotic pressure
3. Increased blood vessel wall permeability e.g.
INFLAMMATION;
4. Obstruction of fluid clearance in the lymphatic
system;
5. Changes in the water retaining properties of the
tissues themselves. Raised hydrostatic pressure often
reflects retention of water and sodium by the kidney
9.
1. INCREASED CAPILLARYHYDROSTATIC
PRESSURE
Rise in hydrostatic pressure at the venular
end of capillaries to a level more than
plasma oncotic pressure
↓
Minimal/ No reabsorption of fluid at
venular end
↓
EDEMA
11.
2. Reduced PlasmaOncotic Pressure
Reduced albumin synthesis in liver /
protein malnutrition
↓
Fall in plasma oncotic pressure
↓
Net movement of fluid into interstitial
tissues
↓
EDEMA
12.
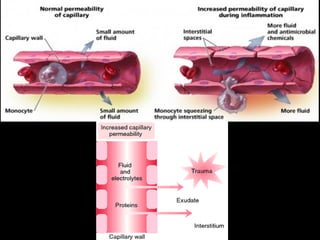
3. INFLAMMATION
Capillary endothelialinjury by toxins/ histamine/
anoxia/ drugs
↓
Endothelial gap
↓
↑ Capillary permeability to plasma proteins
↓
↓Plasma oncotic pressure
↓
EDEMA
14.
4. LYMPHATIC OBSTRUCTION
Impairedlymphatic drainage
↓
Localized LYMPHOEDEMA
(E.g.:-Radical mastectomy for Ca breast;
Pressure on main lymph ducts;
Inflammation of lymphatics;
Occlusion of lymphatics by malignant cells;
Filariasis)
16.
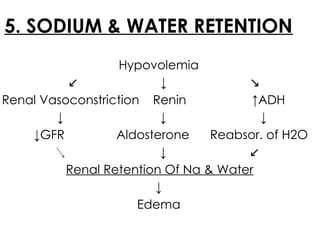
5. SODIUM &WATER RETENTION
Hypovolemia
↙ ↓ ↘
Renal Vasoconstriction Renin ↑ADH
↓ ↓ ↓
↓GFR Aldosterone Reabsor. of H2O
↓ ↙
Renal Retention Of Na & Water
↓
Edema
17.
CLASSIFICATION
Edema can beclassified as GENERALISED or LOCALISED.
• GENERALIZED EDEMA is a condition when you notice
swelling, puffiness, and water retention in various body
parts, including your abdomen, arms, legs, face, and
feet.
• Symptoms include bloating, tightening of skin, and skin
that holds an imprint or looks pitted
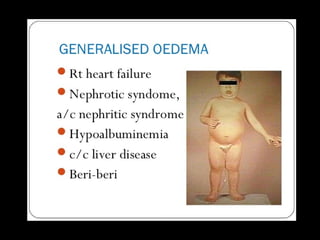
• Conditions leading to generalised edema:
1. Congestive Heart Failure
2. Nephrotic syndrome
3. Cirrhosis of Liver
4. Systemic Infection etc.
19.
• LOCALISED EDEMAcan be defined as the type of
edema confined to a particular part/organ of the
body.
• Various conditions that lead to localised edema
are:
1. Trauma
2. Infection
3. Lymphatic Obstruction like Filariasis
4. Venous Obstruction (e.g.- thrombosis)
21.
Edema can alsobe classified as PITTING or NON-PITTING.
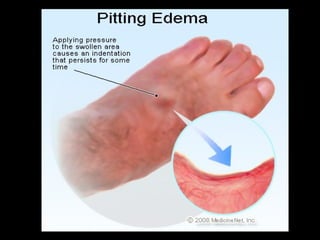
• Cutaneous edema is referred to as “PITTING" when, after
pressure is applied to a small area, the indentation persists
after the release of the pressure.
• Peripheral pitting edema is the more common type,
resulting from water retention. It can be caused by
systemic diseases, pregnancy in some women, either
directly or as a result of heart failure, or local conditions
such as varicose veins, thrombophlebitis, insect bites, and
dermatitis.
• “NON-PITTING EDEMA” is observed when the indentation
does not persist. It is associated with conditions such as
lymphedema, lipedema, and myxoedema.
23.
MAJOR TYPES
There aredifferent types of edema. Some of
them are specific to certain parts of the body,
while others may be more generalized.
Edema can be majorly classified into following
types:
a) PERIPHERAL EDEMA
b) PULMONARY EDEMA
c) CEREBRAL EDEMA
24.
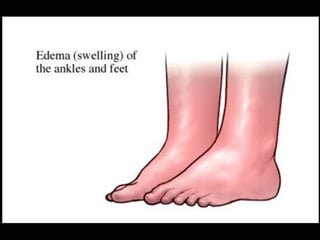
a. PERIPHERAL EDEMA
•Peripheral edema mainly occurs in the legs, feet, and ankles.
This is the most common type of edema and it causes swelling
in the lower extremities.
• This type of edema may be caused by increasing age,
pregnancy, hypertension, congestive heart failure, kidney
problems or other health conditions.
• You also may experience peripheral edema if you have been
sitting or standing for extended hours. Some medications may
also cause peripheral edema:
1. NSAIDs (ibuprofen, naproxen)
2. Corticosteroids (prednisone, methylprednisolone)
26.
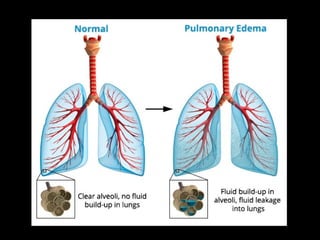
b. PULMONARY EDEMA
•Pulmonary edema is the accumulation of fluids in the lungs
due to the blockage of the pulmonary veins. As blood
pressure rises in the blood vessels of the lungs, fluids rush in to
fill the lungs.
• The pleural cavity can also be filled with fluid. In such cases,
the pulmonary edema is said to also present with pleural
effusion.
• Pulmonary edema is usually caused by the malfunctioning of
the left ventricle of the heart (leads to ↑sed pulm. vein
pressure which causes ↑sed hydrostatic pressure).
• Other causes can be:
a) Acute Respiratory Distress Syndrome.
b) Hypersensitivity Reaction
(Pink Frothy Sputum is the classical symptom of this edema.)
28.
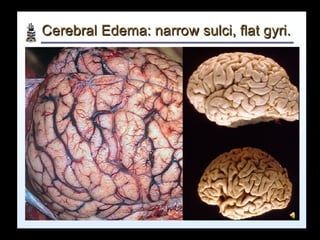
c. CEREBRAL EDEMA
•In cerebral edema, fluids accumulates in the intracellular
and extracellular spaces of the brain. It can be caused by
metabolic abnormalities due to an underlying disease or as
a response to oxygen deprivation at high altitudes.
• Cerebral edema is a very serious form of edema. It can lead
to loss of consciousness and brain damage.
• Cerebral edema can be further divided into 3 subtypes of
edema. These are :
1. Vasogenic
2. Cytotoxic
3. Interstitial cerebral edema.
30.
• Vasogenic cerebraledema occurs when the blood-brain barrier
breaks down. This allows plasma to leak into the brain, first reaching
the white matter before getting to the grey matter. This type of
cerebral edema is caused by tumour, trauma or cardiovascular
events.
• Cytotoxic cerebral edema is caused by the malfunctioning of the
sodium and potassium pump of the glial cells. This leads to the
accumulation of sodium and water and then the swelling of the
gray and white matter. The blood-brain barrier is unaffected in
cytotoxic edema.
• Interstitial edema occurs when the barrier between the brain and
the cerebrospinal fluid ruptures. This causes the inflow of
cerebrospinal fluid into the brain and its accumulation in the white
matter and extracellular spaces.