Download to read offline

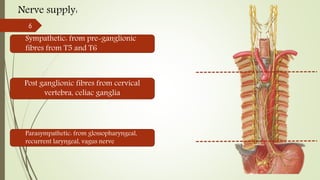
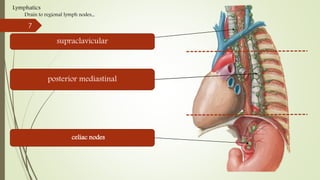






The document provides information on the anatomy, physiology, and pathologies of the esophagus. It discusses the layers of the esophagus, blood supply, nerve supply, and functions like peristalsis. Key pathologies covered include dysphagia, achalasia, gastroesophageal reflux, and esophageal cancer. Esophageal cancer is further discussed in terms of risk factors, staging, and surgical management options like Ivor Lewis esophagectomy.











![Stomach and duodenum_-_benign_lesions[2]](https://cdn.slidesharecdn.com/ss_thumbnails/stomachandduodenum-benignlesions2-171112093735-thumbnail.jpg?width=640&height=640&fit=bounds)



















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)



