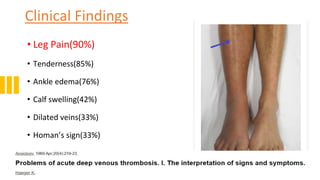
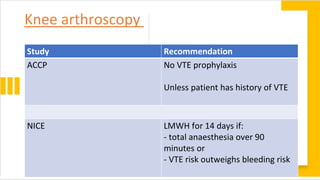
The document discusses prophylaxis for deep vein thrombosis (DVT). It defines DVT and describes its pathophysiology. Risk factors for DVT include surgery, immobilization, old age, cancer, and inherited or acquired thrombophilias. Without prophylaxis, DVT can occur in 40-60% of major orthopedic surgeries and lead to pulmonary embolism. Methods of prophylaxis include mechanical methods like mobilization and compression devices as well as pharmacological methods like low molecular weight heparin, factor Xa inhibitors, and vitamin K antagonists. Guidelines recommend different prophylaxis options based on surgery type and patient risk factors