Download to read offline
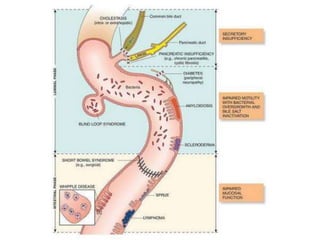
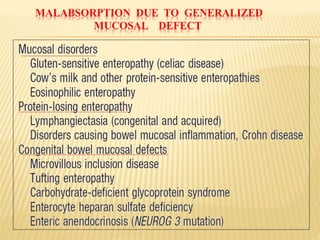
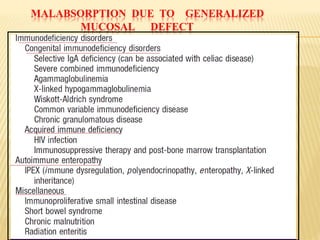
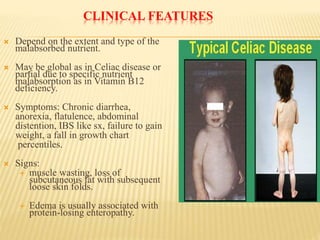
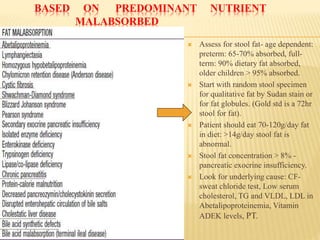
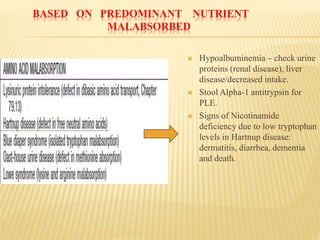
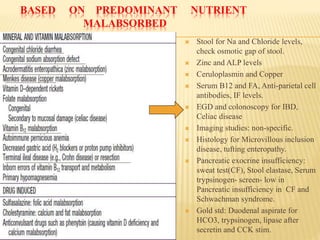
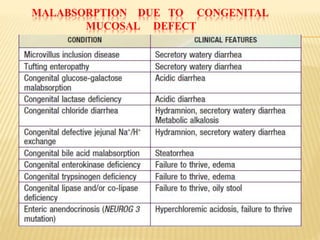


The document discusses malabsorption and maldigestion, detailing their distinct pathophysiological mechanisms and interdependence in nutrient absorption. It covers clinical features, diagnostic approaches, specific disorders, and treatment strategies related to malabsorption in various conditions such as celiac disease, IBD, and congenital defects. Key diagnostic methods include stool tests, biopsies, and clinical assessments, while treatment focuses on addressing nutrient deficiencies and underlying causes.



































































