Malabsorption syndromes encompass numerous clinical entities that result in chronic diarrhea, abdominal distention, and failure to thrive. [1] Clinical malabsorption can be broken down into several distinct conditions, both congenital and acquired, that affect one or more of the different steps in the intestinal hydrolysis and subsequent transport of nutrients.

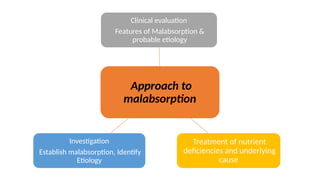
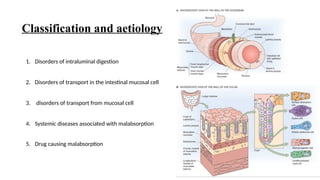
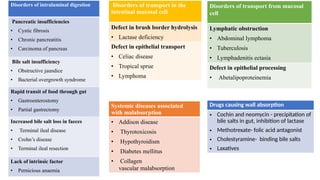
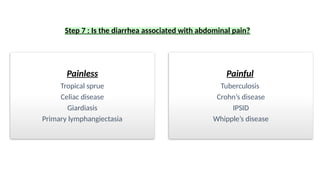



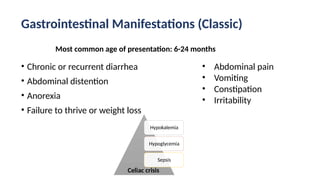












![REFERENCES
1. A Riyaz , Textbook of Paediatric Gastroenterology & Hepatology, 4th
Edition
2. Nelson Textbook of pediatrics, 21st
Edition
3. Sonawane R. ABETALIPOPROTEINEMIA. Pediatr Oncall J. 2016;13: 1-8. doi: 10.7199/ped.oncall.2016.1
4. Siniewicz-Luzeńczyk K, Bik-Gawin A, Zeman K, Bąk-Romaniszyn L. Small intestinal bacterial overgrowth syndrome
in children. Prz Gastroenterol. 2015;10(1):28-32. doi: 10.5114/pg.2014.47494. Epub 2015 Feb 6. PMID:
25960812; PMCID: PMC4411403.
5. Brar HS, Aloysius MM, Shah NJ. Tropical Sprue. [Updated 2023 Jan 30]. In: StatPearls [Internet]. Treasure Island
(FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK567742
6. Nagra N, Dang S. Protein-Losing Enteropathy. [Updated 2023 Jun 12]. In: StatPearls [Internet]. Treasure Island
(FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK542283/](https://image.slidesharecdn.com/approachomalabsorption-1-250729152345-7c9255ec/85/approach-o-malabsorption-in-children-pptx-72-320.jpg)















































