Diarrhoea andweight loss with a normal diet is likely to be
malabsorption.
The symptoms are diverse in nature and variable in severity.
It is also described as syndrome complex but there are specific cause
and pathology that may differ accordingly.
A few patients have apparently normal bowel habit but diarrhoea is
usual and may be watery and voluminous.
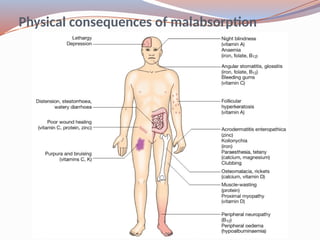
Bulky, pale and offensive stools which float in the toilet (steatorrhoea)
signify fat malabsorption. Abdominal distension, borborygmi, cramps,
weight loss and undigested food in the stool may be present.
Some patients complain only of malaise and lethargy.
3.
Pathophysiology
Malabsorption results fromabnormalities of the three processes
which are essential to normal digestion:
Intraluminal maldigestion occurs when deficiency of bile or
pancreatic enzymes results in inadequate solubilisation and
hydrolysis of nutrients. Fat and protein malabsorption results. This
may also occur with small bowel bacterial overgrowth.
Mucosal malabsorption results from small bowel resection or
conditions which damage the small intestinal epithelium, thereby
diminishing the
surface area for absorption and depleting brush border enzyme
activity.
‘Post
mucosal’ lymphatic obstruction prevents the uptake and
Coeliac disease
Coeliacdisease is an immunologically mediated inflammatory disorder
of the small bowel occurring in genetically susceptible individuals.
Coeliac disease is an immunologically mediated inflammatory disorder
of the small bowel occurring in genetically susceptible individuals.
It is caused by intolerance to wheat gluten and similar.
The precise pathogenesis is unclear but immunological responses
to gluten play a key role.
Tissue transglutaminase (tTG) is now recognised as the autoantigen for
anti
endomysial antibodies.
It is associated with other HLA
linked autoimmune disorders
10.
Infants: failureto thrive, malabsorption.
Children: delayed growth and puberty, malnutrition, abdominal
distension.
Adults: presents in third or fourth or decade; 2 : 1 female predominance.
Florid malabsorption in some; others present with tiredness, weight loss,
iron or folate deficiency. Oral ulceration, dyspepsia and bloating.
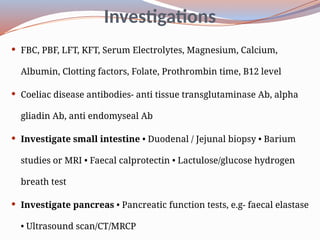
Duodenal or jejunal biopsy: Villous atrophy is characteristic.
Antibodies: - anti tissue transglutaminase Ab, alpha gliadin Ab, anti
endomyseal Abtests are not a substitute for small bowel biopsy; they
usually become negative with successful treatment.
● Lifelong gluten free diet. Correction of deficiencies of iron, folate,
●
calcium and vitamin D.
11.
Tropical sprue
Tropicalsprue is a chronic, progressive malabsorption with abnormalities
of small intestinal structure and function occurring in the tropics.
The disease occurs mainly in the West Indies and in Asia, including
southern India, Malaysia and Indonesia.
It often begins after an acute diarrhoeal illness. Small bowel bacterial
overgrowth with Escherichia coli, Enterobacter and Klebsiella is frequently
seen. Mucosal pathology closely resembles that of coeliac disease.
Clinical features include: Diarrhoea, abdominal distension, anorexia,
●
fatigue and weight loss. Onset of severe diarrhoea: may be sudden.
●
When chronic: Megaloblastic anaemia (folic acid malabsorption).
● ●
Ankle oedema, glossitis and stomatitis. Remissions and relapses: may
●
occur.
Tetracycline (250 mg 4 qds for 28 days) brings long term remission or cure.
12.
Whipple’s disease
Thisrare condition is characterised by infiltration of small intestinal
mucosa by ‘foamy’ macrophages, which stain positive with periodic acid–
Schiff (PAS) reagent. The cause is infection of macrophages by Gram
positive
bacilli (Tropheryma whipplei), detectable in biopsies by PCR.
Middle
aged men are most commonly affected and the presentation
depends on the pattern of organ involvement. Low-grade fever is common.
Whipple’s disease is often fatal if untreated but responds well to 2 wks of IV
ceftriaxone followed by co
trimoxazole for at least a year. Relapse occurs in
up to one third of patients, often within the CNS.
13.
Bacterial overgrowth (‘blindloop syndrome’)
The normal duodenum and jejunum contain coliform organisms, but
numbers never exceed 103/mL. In bacterial overgrowth there may be 108–
1010/mL organisms, most of which are normally found only in the colon.
Disorders that predispose to bacterial overgrowth include hypochlorhydria,
impaired motility (e.g. systemic sclerosis, diabetes), surgical resection,
fistulae and hypogammaglobulinaemia.
Clinical features include: Watery diarrhoea and/or steatorrhoea.
● ●
Anaemia due to vitamin B12 deficiency. There may also be symptoms from
the underlying intestinal cause.
14.
Investigations- Serumvitamin B12 concentration is low; folate levels
●
are normal or elevated. Ig levels: may exclude
●
hypogammaglobulinaemia. Barium follow
through or small bowel
●
enema: may reveal blind loops or fistulae. Endoscopic duodenal
●
biopsies: exclude mucosal disease such as coeliac disease. Endoscopic
●
aspiration of jejunal contents: for anaerobic and aerobic culture. ●
Hydrogen breath test.
Management is of the underlying cause. Tetracycline is the treatment of
choice, although up to 50% of patients do not respond. Metronidazole or
ciprofl0xacin is an alternative.
Some patients require up to 4 wks of treatment and a few cases become
chronic. IM vitamin B12 supplementation is needed in the latter.
15.
Short bowel syndrome
Malabsorption resulting from extensive small intestinal resection or disease.
Loss of surface area for digestion and absorption is the key problem.
Clinical features include: Large
volume jejunostomy fluid loss. If colon is
● ●
preserved: diarrhoea and steatorrhoea. Dehydration and signs of
●
hypovolaemia. Weight loss, loss of muscle bulk and malnutrition.
●
Management entails: Total Parenteral Nutrition PPI therapy: to reduce
● ●
gastric secretions. Enteral feeding: to be cautiously introduced after 1–2
●
wks and slowly increased as tolerated.
Long
term management are: Detailed nutritional assessments.
● ●
Monitoring of fluid and electrolyte balance. Adequate calorie and protein
●
intake. Replacement of vitamin B12, calcium, vitamin D, magnesium, zinc
●
and folic acid. Antidiarrhoeal agents, e.g. loperamide or codeine
●
phosphate.
16.
Ileal resection
Ilealresection is usually performed as treatment for Crohn’s disease.
The long
term effects depend on the site and the length of intestine
resected, and vary from trivial to life threatening.
Clinical features include:
Diarrhoea. Fat malabsorption due to loss of bile salts. Gallstones
● ● ●
due to lithogenic bile. Oxalate renal calculi. Vitamin B12 deficiency.
● ●
Contrast studies of the small bowel and tests of vitamin B12 and
bile acid absorption are useful.
Parenteral vitamin B12 supplementation is necessary.
Diarrhoea responds to colestyramine or aluminium hydroxide therapy.

































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



