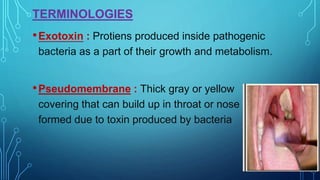
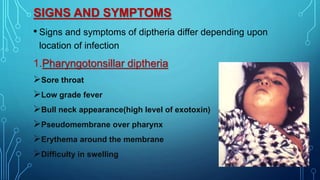
Diphtheria is a highly infectious and communicable disease caused by the bacterium Corynebacterium diphtheriae, primarily affecting the throat and upper airways. It is characterized by the production of a potent toxin that leads to symptoms such as sore throat, fever, and the formation of a pseudomembrane. Early detection and treatment, along with vaccination, are crucial for prevention and control.