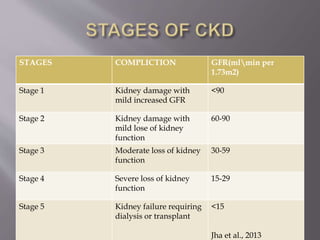
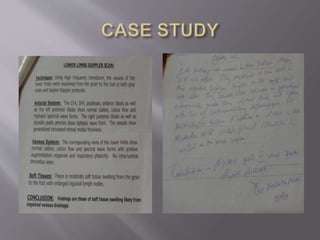
Diabetic nephropathy is a complication of diabetes that results in chronic kidney disease. It is caused by damage to the glomeruli of the kidneys from hyperglycemia. It can progress to kidney failure if not controlled. The presentation includes edema, hypertension, reduced kidney function. Management involves controlling blood sugar and pressure with medications like ACE inhibitors. Prognosis depends on stage of disease and risk factors present, with proteinuria indicating higher mortality risk. Physiotherapy can help reduce pain and swelling and improve function for patients with diabetic nephropathy.





























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



