Downloaded 82 times





























![ Occurrence of coma in diabetic patients in theOccurrence of coma in diabetic patients in the
absence of definitive elevation of effectiveabsence of definitive elevation of effective
osmolality ≥320 mOsm/kg demandsosmolality ≥320 mOsm/kg demands
immediate consideration of other causes ofimmediate consideration of other causes of
such change.such change.
Effective osmolality may be calculated by theEffective osmolality may be calculated by the
following formula:following formula:
2[measured Na (mEq/l)] + glucose (mg/dl)/182[measured Na (mEq/l)] + glucose (mg/dl)/18](https://image.slidesharecdn.com/diabeticketoacidosis-150115224933-conversion-gate02/75/Diabetic-ketoacidosis-31-2048.jpg)





































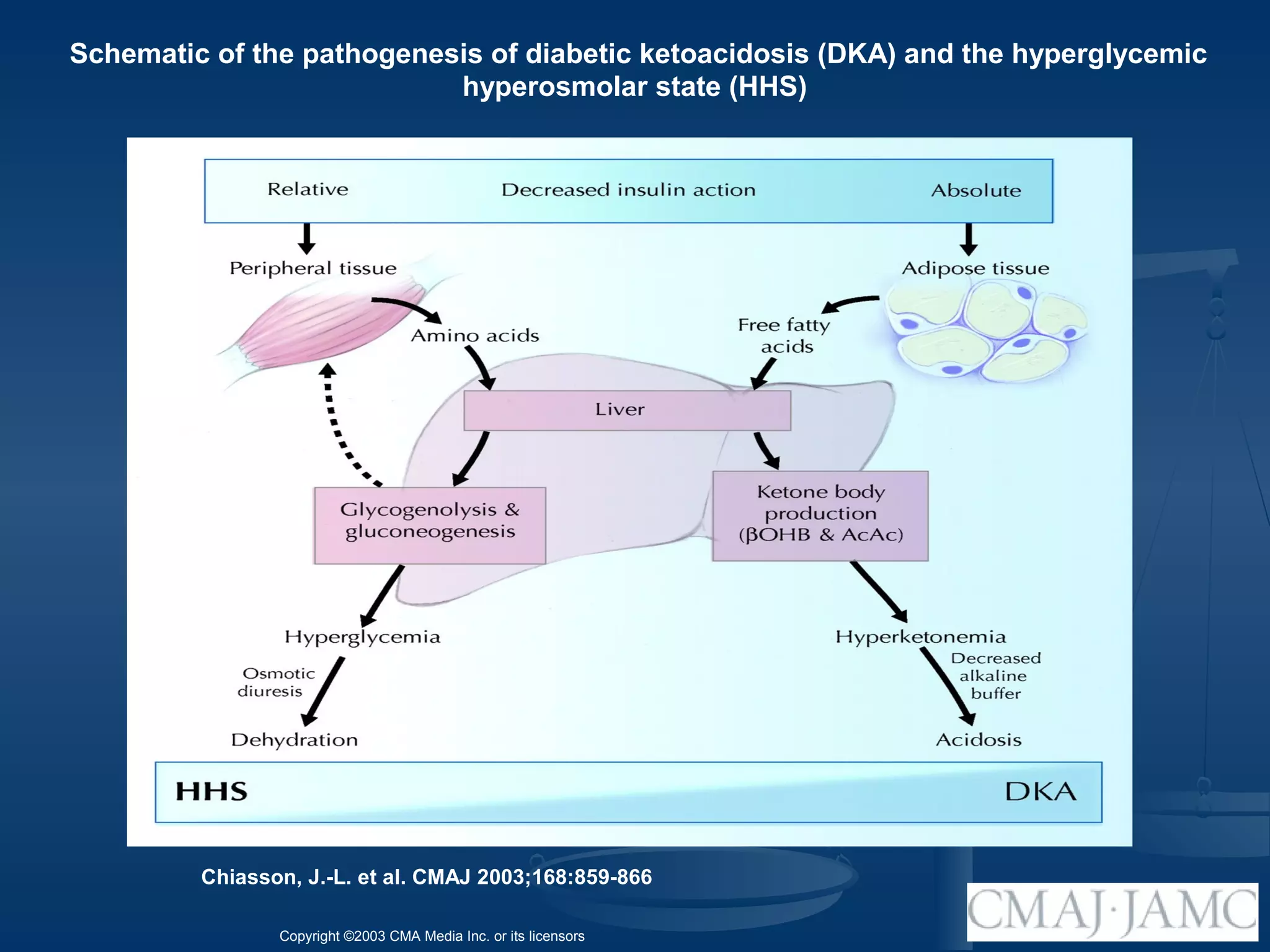
This document discusses diabetic ketoacidosis (DKA). It defines DKA as a metabolic acidosis caused by the accumulation of ketones from severely low insulin levels. Key characteristics of DKA include hyperglycemia, low bicarbonate, acidosis, and ketonemia/ketonuria. The document outlines the pathophysiology of DKA, including how low insulin and high glucagon levels lead to increased ketone production and acidosis. Clinical presentation of DKA is also described.
























































































