

![Fluid conservation:
• Clofibrate (Atromid-S), a hypolipidemic agent, has been
found to have an antidiuretic effect on patients who have
some residual hypothalamic vasopressin.
• Chlorpropamide (Diabinese) and thiazide diuretics are also
used in mild forms of the disease because they potentiate the
action of vasopressin.
• Thiazide diuretics, mild salt depletion, and prostaglandin
inhibitors (ibuprofen [Advil, Motrin], indomethacin
[Indocin], and aspirin) are used to treat the nephrogenic form
of diabetes insipidus.](https://image.slidesharecdn.com/diabeticincipidus-230115134048-06689ccc/85/diabetic-incipidus-pptx-23-320.jpg)


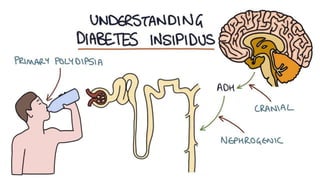
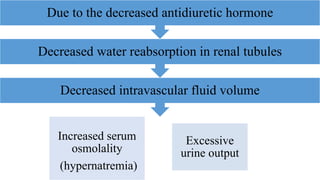
This document provides an overview of diabetes insipidus (DI), including defining the condition as a deficiency of antidiuretic hormone resulting in excessive thirst and urine production. It discusses the objectives of teaching about DI, risk factors, types of DI, clinical manifestations involving polyuria and polydipsia, pathophysiology of increased serum osmolality, assessment, management involving vasopressin replacement and fluid conservation, nursing management, monitoring, self-care, and references research studies on DI.