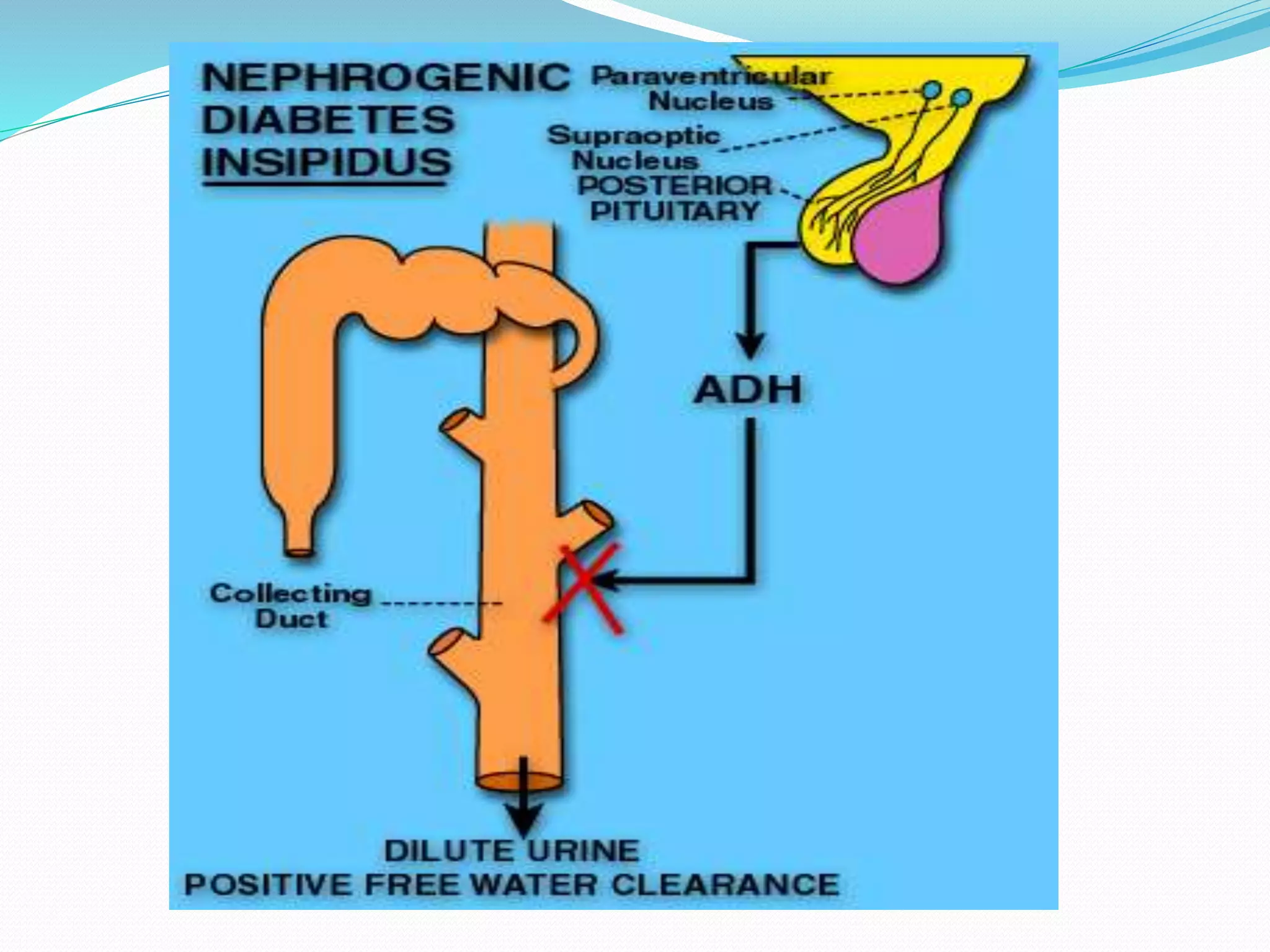
Diabetes insipidus is a disorder characterized by excessive urine production and thirst due to a deficiency of antidiuretic hormone. There are two main types: central diabetes insipidus caused by issues with the pituitary gland, and nephrogenic diabetes insipidus caused by kidney problems. Symptoms include producing large volumes of dilute urine, excessive thirst, and dehydration. Treatment aims to replace ADH through medications like DDAVP, correct fluid and electrolyte imbalances, and identify and address the underlying cause of the condition.