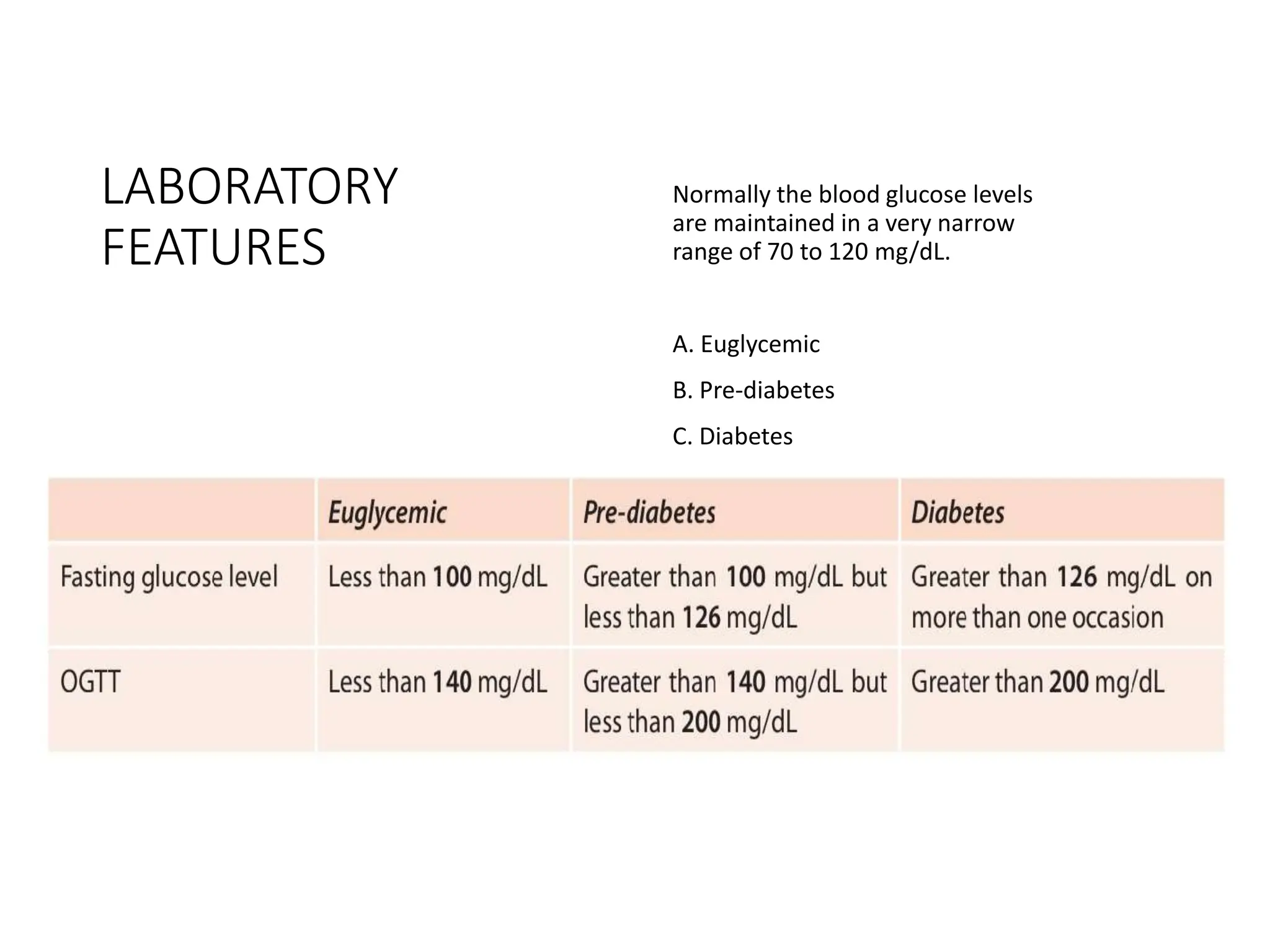
Type 2 diabetes is characterized by insulin resistance and impaired insulin secretion leading to hyperglycemia. It accounts for 90-95% of diabetes cases and is associated with obesity, physical inactivity, and genetic factors. The pathogenesis involves both insulin resistance in tissues and a relative insulin deficiency due to beta cell dysfunction. Clinical features include polyuria, polydipsia, and weight loss, and diagnosis is based on elevated blood glucose levels. Treatment focuses on lifestyle changes and medication to control blood sugar and prevent complications affecting organs like the eyes, kidneys, and nerves.