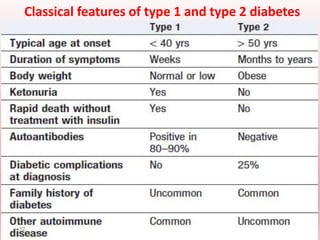
This document summarizes diabetes mellitus and its management. It defines diabetes as a clinical syndrome characterized by hyperglycemia. The two most common types are type 1, caused by autoimmune destruction of insulin-producing cells, and type 2, characterized by insulin resistance and inability to produce sufficient insulin. Environmental and genetic factors contribute to both types. Symptoms, diagnosis, and treatment options like diet, medications, and insulin are discussed in detail. The goals of management are to improve hyperglycemia symptoms and minimize long-term complications through glycemic control.