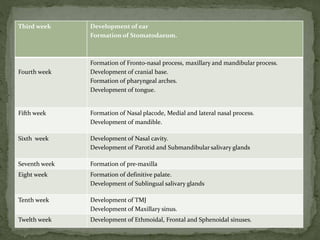
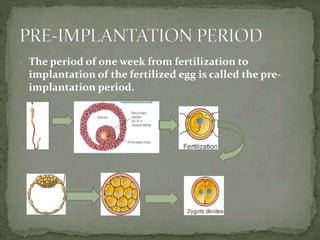
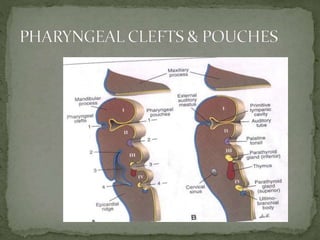
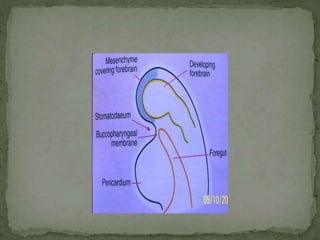
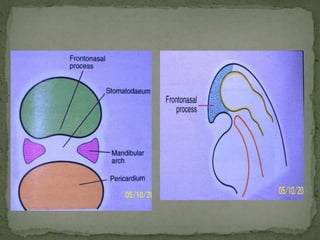
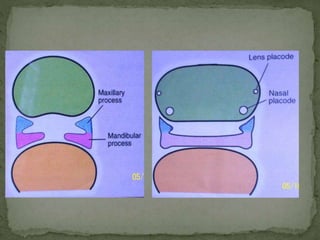
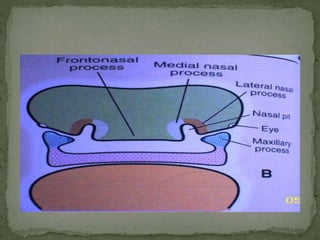
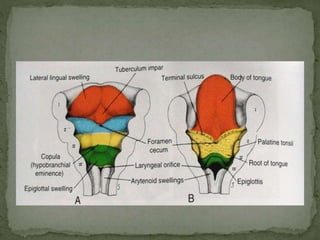
The document discusses the stages of human embryological development, specifically focusing on the formation of facial structures and associated anatomical components. It details the timeline of development from fertilization through various embryonic stages, touching upon the formation of key features such as the face, mouth, and associated structures, as well as potential developmental anomalies. Additionally, it outlines specific components and functions of branchial arches, tongue development, and the formation of salivary glands.
















































![SecurityBoat_Service_Pitch_Deck[24158].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/securityboatservicepitchdeck24158-260121113056-452683e3-thumbnail.jpg?width=640&height=640&fit=bounds)















