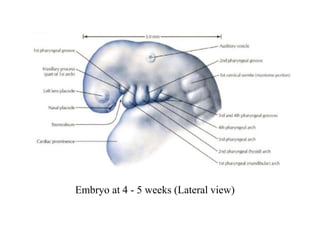
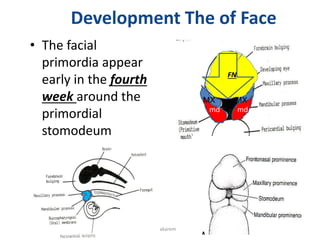
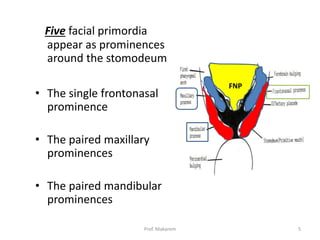
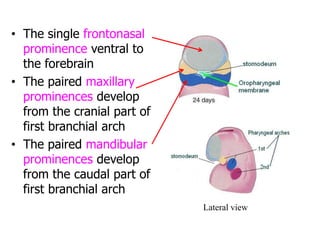
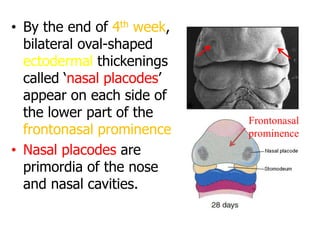
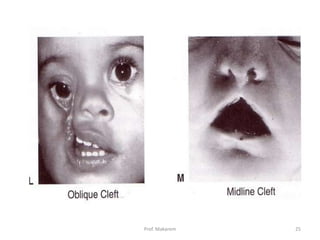
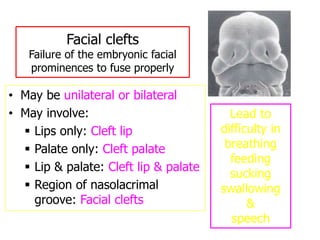
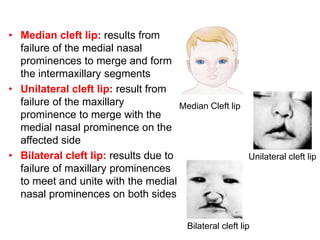
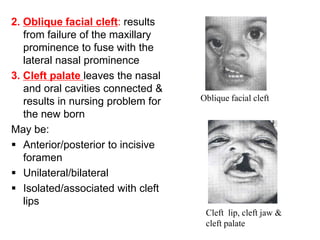
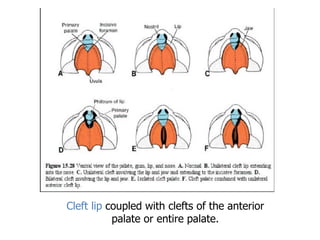
The development of the face occurs mainly between 5-8 weeks of gestation. The lower jaw forms first at 4 weeks, while facial proportions develop between 9 weeks to birth. During infancy and childhood, growth of teeth and sinuses further shapes the face. The five facial primordia - frontonasal, paired maxillary, and paired mandibular prominences - appear by 4 weeks and merge to form the lips, nose, and upper jaw. The nose, nasal cavities, and palate develop from these prominences between 4-12 weeks. Facial anomalies can result if the prominences fail to fuse properly, leading to cleft lips, cleft palates, or other clefts.