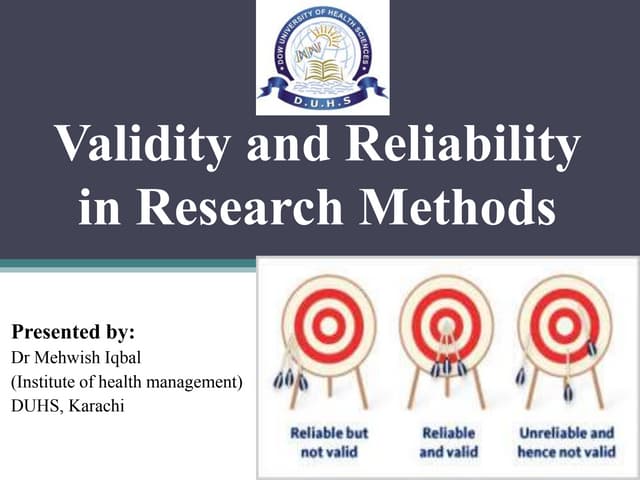
This document discusses various methods used to define diagnostic test results as normal or abnormal. It describes qualitative and quantitative tests, and issues with defining normals based on cultural opinions, percentiles, or presence of risk factors. Common statistical approaches like normal distribution curves and their limitations are explained. The document also covers predictive value, using multiple tests, and receiver operating characteristic curves to evaluate diagnostic tests.